No laws or policies reviewed address consent from a third party when youth are accessing FP services; therefore, Bangladesh is placed in the gray category for this indicator.
The
Bangladesh Essential Health Service Package (ESP), 2016
guidelines for screening for contraceptive use direct providers to follow medical eligibility criteria when clients seek FP services. Additional policies outline plans to train providers to provide non-judgmental services to adolescents, but no policies explicitly require providers to authorize medically advised youth FP services without personal bias or discrimination. Bangladesh is placed in the yellow category for this indicator.
The
National Strategy for Adolescent Health, 2017-2030" affirms adolescents
right to health regardless of their age as guaranteed by the Constitution of Bangladesh:
Universality and Inalienability
The right to health will be universal and inalienable for all adolescent boys and girls of Bangladesh. They will be entitled to access health related information and services regardless of their gender, age, class, caste, ethnicity, religion, disability, civil status, sexual orientation, geographic divide or HIV status.
Indivisibility
The right of adolescents to their health has equal status over other rights and will not be positioned in a hierarchical order. The right to adolescent health will not be compromised at the expense of other rights.
The
Bangladesh Population Policy 2012
acknowledges the need to bring adolescents under family planning coverage to improve client-centered services but fails to state that adolescents should have access to FP regardless of age:
- Major Strategies for Implementation of the Population Policy
5.1 Client-Centred Service
Improve service centre practices and door-to-door services to ensure client-centred services, and undertake the following strategies to make them complement each other:
d) bring newlyweds, adolescents, and parents of one or two children under the coverage of family planning services on a priority basis.
Though Bangladesh
s policies support adolescents
right to health and promote client-centered services, they do not include language that explicitly supports youth access to FP services regardless of age. Bangladesh is therefore placed in the gray category for this indicator.
The
National Strategy for Adolescent Health, 2017-2030" refers to a regulation that makes sexual and reproductive health services available only to married women and eligible couples:
Finally it is important to address the issue of unmarried adolescents, who fall outside the existing reproductive health care services system, given the regulation that SRH [sexual and reproductive health] services are available only to married women and eligible couples.
While this regulation could not be identified by name and could not be located, the Strategy then acknowledges the importance of making SRH services, including family planning, accessible to all adolescents regardless of their marital status but does not detail any strategic objectives to reach this goal:
Given...the significant population of adolescents in Bangladesh, where a majority of adolescent girls are given in marriage before the age of 18 years, meeting the sexual and reproductive health needs and rights of this group becomes imperative. These needs can be met by ensuring the provision of quality and age appropriate sexuality education starting with the very young adolescent, the delivery of quality age and gender appropriate SRH information and services and mobilization of the community to accept the importance of meeting the SRH and rights of all adolescents, irrespective of their marital status.
The
Costed Implementation Plan for National Family Planning Program in Bangladesh, 2020-2022" also alludes to a regulation restricting family planning to married couples and specifically targets newly married couples in plans to scale-up FP counseling and services. Furthermore, the plan specifically includes an activity to provide contraception to the
bridegroom/bride,
with no comparable activity targeting unmarried adolescents.
As Bangladesh
s existing policy regulations restrict access to SRH services based on marital status and more recent policies do not go far enough to remove this barrier, Bangladesh is placed in the red category for this indicator.
The
Clinical Contraception Services Delivery Programme Operational Plan, 2011-2016
notes that Bangladesh
s family planning programs use medical eligibility criteria based on World Health Organization (WHO) guidelines:
Medical Eligibility Criteria for Contraceptive use has been developed in perspective of national FP programme of Bangladesh based on WHO guidelines. This criteria has been included in the FP manual. These will help in proper client screening in reducing drop-outs, side-effects/ complications and unnecessary method-switching. At the same time every effort will be made to increase the accessibility of FP users in facilities by making those more attractive and user-friendly by improving provider attitude and management of FP services through proper counseling and screening.
The Operational Plan notes that the FP manual was undergoing an update, but the update could not be accessed at the time of analysis.
As part of its strategy to target adolescents, the
Costed Implementation Plan for National Family Planning Program in Bangladesh, 2020-2022
includes an activity to ensure contraceptive availability, including long acting reversible contraceptives (LARCs), for all adolescents:
7.5 Making all services (both short and LARC) available for the adolescents in the facilities.
Phasing of adolescent friendly contraceptive services
7.5.1 Ensure availability of the logistics at all level (No additional cost required)
The
Bangladesh Essential Health Service Package (ESP), 2016
acknowledges that adolescent health covers
distribution of condoms
and
FP information and provision,
but it does not detail method eligibility for adolescents and youth. The Service Package continues to note that screening for contraceptive use follows medical eligibility criteria but provides no further detail.
The Service Package does not explicitly state that these methods are available regardless of age, parity, and marital status, and the Costed Implementation Plan is the only policy document reviewed that mentions the need to ensure the availability of contraceptives , including LARCs, to adolescents. Bangladesh is therefore placed in the yellow category for this indicator.
Although the availability of emergency contraception (EC) is not factored into the categorization of this indicator, it is worth noting that Bangladesh
s policies do not specify whether access to EC should be available to adolescents.
The
National Plan of Action for Adolescent Health Strategy, 2017-2030" includes a strategic objective to integrate age-appropriate comprehensive sexuality education (CSE) at all educational levels:
Key Strategy: Promote age appropriate comprehensive
sexuality education, which are on par with international standards, through all academic and training instructions.
Major Activities:
- Revise Secondary School and Madrasah Curriculum (Class VI-X) to strengthen the CSE component Include adolescent development and CSE contents in B. Ed. course Conduct Peer Educator training (2 students from each school)
The Plan of Action also mentions CSE in its section focused on adolescent mental health:
Key Strategy: Develop skills among adolescents to deal with stress, manage conflict, and develop healthy relationships.
Major Activities:
- Organize sessions on Comprehensive
Sexuality Education (CSE)/Life Skills Education/(LSE) for adolescents
through the SHP [sexual health program], AH [adolescent health] clubs
- Provide training on LSE.
However, the Plan of Action does not provide guidance or details on the specific components of the CSE curriculum or which students will be targeted.
Multiple policies and operational plans address improving knowledge of sexual and reproductive health (SRH) in schools and community settings without providing further details. The
National Children Policy, 2011
acknowledges the need to include information on reproductive health in the school syllabus. The
Costed Implementation Plan for National Family Planning Program in Bangladesh, 2020-2022" includes an activity to incorporate an adolescent health program into the school curriculum. The
Maternal, Neonatal, Child, and Adolescent Health Operational Plan, 2017-2022" includes effective dissemination of SRH knowledge and information through school curricula and community-based dissemination. The Operational Plan also includes an activity to link schools to SRH services, although it provides no detail on whether these linkages are also promoted in the curriculum:
Component 4: Adolescent Health
Activities:
- Establishment of referral linkages between school health clinics and other health facilities.
While the
Bangladesh Population Policy, 2012
includes adolescent SRH education activities, including dissemination workshops on family planning for adolescents in schools and colleges and life skills education, these activities specifically target married adolescents.
The
National Education Policy, 2010
outlines aims and objectives of education in Bangladesh and lays out additional aims, objectives, and strategies for different levels (primary, adult, secondary, vocational, etc.) and types of education (such as science, business, and engineering). The policy includes a section on
Women
s Education,
which aims to continue women
s access to education to ensure future development and economic participation and includes a strategy to include reproductive health in the curriculum:
The secondary level curriculum of last two years will include gender studies and issues of reproductive health.
Similarly, a draft version of the
National Youth Policy, 2017
aims to include life skills and education on sexual and reproductive health and rights in the curriculum, but does not outline any further steps or details on recipients or curriculum content:
Include sexual and reproductive health and rights to sexual and reproductive health in the curriculum.
9.1.9 Build awareness among youth about reproductive health, rights to reproductive health and about sexual health
10.5.3 Equip youth with greater sensibility to violation of human rights anywhere in the society or against any group or community, and motivate them to play an active role in the case of such occurrences.
The
National Communication Strategy for Family Planning and Reproductive Health, 2008,
which is designed to serve as a roadmap for increasing knowledge, improving attitudes, and changing behaviors related to family planning and reproductive health, outlines various approaches to reaching its goal among different target audiences
including adolescents and unmarried youth. Neither approach provides details on a CSE curriculum, but both address the need to increase FP knowledge and awareness about gender equity:
Audience 5: Adolescents
Sub-objectives:
- Increase the number of adolescents that have correct knowledge about their bodies, and can practice proper hygiene;
- Encourage dialogue between parents and children about marriage, fertility, reproductive health, maternal health;
Audience 6: Unmarried Youth
Sub-objectives:
- Increase awareness among youth (in-school and out-of-school) about the negative effects of gender-based violence;
- Increase knowledge about (gender-specific) sexual health rights;
- Improve the reach of life-skills/family life education programs to include greater numbers of out- of-school youth;
- Increase knowledge about sexual responsibility;
- Increase the number of unmarried youth that delay age at marriage;
- Increase the number of unmarried youth that know the advantages to having no more than two children;
- Increase the number of unmarried youth that have a positive attitude
toward family planning
While Bangladesh
s policy environment acknowledges the need for CSE and SRH education in schools, no policy documents provide further details on the content of a curriculum or outline detailed activities that would support UNFPA's essential components of CSE. Bangladesh is therefore placed in the yellow category for this indicator.
In its priority area targeting adolescents and youth, the
Costed Implementation Plan for National Family Planning Program in Bangladesh, 2020-2022
includes activities to train providers to withhold judgment and ensure confidentiality and privacy for youth seeking services:
7.2 Training of providers on adolescent friendly services (AFS10) with privacy and confidentiality
FWVs [family welfare visitors] and SACMOs [sub-assistant community medical officers] focusing on providing non-judgmental services, accurate information on medical eligibility, communication strategy for adolescents.
7.3 Ensuring private and confidential counselling room with doors and window curtains, partitioning the waiting areas so that adolescents
clients do not have to mix adult clients, not conducting history taking and screening in public
7.4 Developing adolescent friendly communication materials and digital health services.
7.5 Making all services (both short and LARC [long-acting reversible contraceptives]) available for the adolescents
in the facilities, phasing of adolescent friendly contraceptive services.
The "National Strategy for Adolescent Health, 2017-2030" acknowledges the need to take into consideration
issues of affordability and accessibility of health services
for vulnerable adolescents and calls for a key focus on making contraceptives and services available to youth for free or at low cost.
The
National Plan of Action for Adolescent Health Strategy, 2017-2030" includes an activity to train providers on adolescent friendly health services and counseling:
Key Strategy: Build capacity for the delivery of age and gender sensitive sexual and reproductive health services which includes HIV/STI prevention, treatment and care.
Major Activities:
- Develop and update comprehensive training module on AFHS [adolescent-friendly health services] and Counselling (including family planning) for Service Providers and Field Workers.
- Organize [Training of Trainers] for Master trainers
- Conduct training of Service Providers and Field Workers in the provision of Adolescent Friendly Health Services and Counselling, particularly on Family planning.
- Review the medical and pre-service training curriculum of health workers (doctors, nurses, midwives, paramedics and field workers) to ensure the inclusion of adolescent health and counselling with special focus on Family planning
The Plan of Action further notes the need to train providers to adopt non-judgmental attitudes when working with adolescents in its section on health systems strengthening:
Key Strategy HWF [Health Work Force] 1: Capacity building of health providers to be sensitive to the needs of all adolescents, including those who are unmarried, through pre service, in service and on the job training;
Major Activities:
- Development of [Management Information System] for HR [human resources] Management and for gap analysis
- Training and mentoring all [healthcare providers]
on [adolescent health] and rights related issues including special health needs by providing pre- and in-service trainings
- Development of Course on Adolescent Health and incorporate it in post-graduation
Key Strategy HWF 2: Provide health service personnel with training on counselling for adolescents
and capacitate them to adopt non-judgmental attitudes when working with adolescents.
Major activities:
- Deployment of human resource to provide adolescent health services based on need
- Train [healthcare providers] on psychosocial counselling, family planning, gender diversity and value clarification issues.
Moreover, the
National Communication Strategy for Family Planning and Reproductive Health, 2008
includes a specific objective to
improve the attitudes of service providers toward adolescents and youth with regard to family planning and reproductive health seeking behavior.
Furthermore, the
Community-Based Health Care Operational Plan, 2017-2022" outlines an implementation process to develop adolescent counseling corners to provide adolescent-friendly services.
Additionally, the
Eighth Five Year Plan, 2020-2025
includes establishing 200 additional adolescent-friendly service centers among the main activities listed for family planning. While the plan aims to ensure the availability of modern contraceptives at a low cost, especially in remote areas, it does not specifically plan for youth
s access to services for free or at reduced costs.
By including provider training for youth-friendly FP services and activities to ensure privacy for youth accessing FP information and services, Bangladesh has fostered a promising policy environment. Bangladesh is placed in the yellow category for this indicator and can further improve its policy environment by ensuring FP services for youth for free or at a reduced cost.
The
Costed Implementation Plan for National Family Planning Program in Bangladesh, 2020-2022
outlines a list of activities to foster a supportive environment for adolescents
family planning and address gender norms, especially targeting parents, religious leaders, public representatives, local elites, providers, etc.:
Strategy 2- Increasing acceptability of LARC&PM [long-acting reversible contraceptives and permanent methods] through skilled HR [human resources] and engaging males
Activities:
2.5 Use satisfied clients/champions for the promotion of LARC&PM in the community
2.7 Use religious leader for the promotion of LARC&PM: Extensive workshops to sensitize religious leaders (Note: even though these strategies are in place as stated in FP OPs[operational plans], field observation suggested that they were not effectively implemented)
...
Strategy 8- Targeting adolescents with special focus on males
Activities:
8.1 Counsel adolescent, newly married couple, in-laws, public representatives and local elites to improve gender norms.
8.5 Counsel and meetings for parents, providers, religious leaders, and other influential adults (public representatives and local elites etc.) who can foster a supportive environment in health
facilities, schools, places of worship, and in homes
To address underlying barriers to adolescent FP access, including community stigma associated with being sexually active, the
National Plan of Action for Adolescent Health Strategy, 2017-2030" acknowledges the need for social and behavior change communication programs to change community attitudes and behaviors and lays out three strategies:
Strategic Objectives
3. To use Social and Behavioral Change Communication [SBCC] interventions to bring about changes in knowledge, attitudes and practices among specific audiences.
Key Strategies
- Development of messages and materials for communication and advocacy through sound research;
- Utilize ICT [information and communications technology] (including call centres) and media to reach adolescents, key community members, parents and guardians;
- Develop the capacity of respective institutions and systems to design, plan, implement and monitor SBCC interventions.
The
National Communication Strategy for Family Planning and Reproductive Health, 2008
lists specific activities to create an enabling social environment for unmarried youth
s access to family planning information and gender equity:
- Engage Imams to discuss reproductive health issues with youth;
- Conduct discussion groups with trained facilitators where youth can learn about, and practice, problem-solving skills with regard to family planning and reproductive health decision-making;
- Educate community gatekeepers (parents, teachers, religious leaders, etc.) about gender equity issues.
The
Maternal, Neonatal, Child, and Adolescent Health Operational Plan, 2017-2022" includes an objective to
create positive change in the behavior and attitude of the gatekeepers of adolescents towards reproductive health.
The plan outlines two relevant strategies to create an enabling social environment:
Advocacy meeting at community level for the gatekeepers of adolescents
...
Carry out multi-sectoral advocacy for creation of supportive environment for adolescents to practice safe behaviors
The Operational Plan does note the specific methods for community mobilization of gatekeepers, but does not go into much detail:
Community mobilization around ASRH [adolescent sexual and reproductive health]
issues through court yard meetings, inter-personal communication, and workshops, through partnership with NGOs, to sensitize gatekeepers (parents, religious leaders, community leaders, school teachers, school management committees. etc.)
The
National Women Development Policy, 2011,
National Education Policy, 2010,
and
Eighth Five Year Plan, 2020-2025,
aim to establish gender equality, promote girl
s education, and ensure equal gender rights in family planning decision-making.
Since Bangladesh
s policy environment details activities to create an enabling social environment for youth access to family planning information and services and addresses gender norms, Bangladesh is placed in the green category for this indicator.
The right to non-discrimination in the
Loi n
2003-04 du 03 mars 2003 relative
la sant
sexuelle et
la reproduction
states that parental and partner consent is not required for patients to receive reproductive health care:
L
autorisation du partenaire ou des parents avant de recevoir des soins en mati
re de sant
de la reproduction peut ne pas
tre requise, pourvu que ce proc
ne soit pas contraire
La loi.
Benin is placed in the green category for this indicator because its policies adequately prohibit parental and spousal consent.
The
Plan d
action national budg
de planification familiale du B
nin, 2019-2023
acknowledges that provider bias toward young people, particularly those who are unmarried, is a pervasive issue preventing young people from accessing family planning (FP) services:
Quant aux adolescents et jeunes non en union, ils craignent de rencontrer leurs parents et les autres adultes dans les points d
la PF et jugent que leur utilisation de la PF est mal per
ue par les prestataires qui pr
rent offrir les m
thodes uniquement aux femmes en union.
The
Strat
gie nationale multisectorielle de la sant
sexuelle et de la reproduction des adolescents et jeunes, 2018-2022
includes an initiative to establish youth-friendly health centers that follow global standards for quality health care services for adolescents and youth. The standards note that adults
judgement of what is best for adolescents should not supersede their obligation to respect youth rights as outlined in the International Convention on the Rights of the Child, but the standards do not specifically address providers or youth access to family planning.
Benin
s policies, however, do not explicitly state that providers must refrain from applying their personal biases and beliefs when providing FP services to youth. Therefore, Benin falls into the gray category for this indicator.
The
Loi n
2003-04 du 03 mars 2003 relative
la sant
sexuelle et
la reproduction
supports individuals
access to reproductive health care regardless of age:
Article 2 : Caract
re universel du droit
la sant
de la reproduction.
Le droit
la sant
de reproduction est un droit universel fondamental garanti
tout
tre humain, tout au long de sa vie, en toute situation et en tout lieu. Aucun individu ne peut
tre priv
de ce droit dont il b
ficie sans aucune discrimination fond
e sur l
ge, le sexe, la fortune, la religion, l
ethnie, la situation matrimoniale.
Article 7 : Droit
la non-discrimination.
Les patients sont en droit de recevoir tous les soins de sant
de la reproduction sans discrimination fond
e sur le sexe, le statut marital, le statut sanitaire ou tout autre statut, l
appartenance
un groupe ethnique, la religion, l
ge ou l
habilit
payer.
The
Loi n
2015-08 portant code de l
enfant en r
publique du B
states that individuals under age 18 have the right to access to reproductive health services:
Article 156 : Sant
de la reproduction de l
enfant
L
enfant doit avoir acc
la sant
de la reproduction sans aucune forme de discrimination, de coercition ou de violence. Il a le droit
information la plus compl
te sur les avantages et les inconv
nients de la sant
de la reproduction, sur les m
thodes de planification familiale et de contraception ainsi que sur l
efficacit
des services de sant
sexuelle et reproductive.
Benin is placed in the green category for this indicator because the policy environment confirms that youth must be permitted access to family planning services regardless of age.
The
Loi n
2003-04 du 03 mars 2003 relative
la sant
sexuelle et
la reproduction
supports individuals
access to reproductive health care, which includes family planning, regardless of marital status:
Article 2 : Caract
re universel du droit
la sant
de la reproduction.
Le droit
la sant
de reproduction est un droit universel fondamental garanti
tout
tre humain, tout au long de sa vie, en toute situation et en tout lieu. Aucun individu ne peut
tre priv
de ce droit dont il b
ficie sans aucune discrimination fond
e sur l
ge, le sexe, la fortune, la religion, l
ethnie, la situation matrimoniale.
Article 7 : Droit
la non-discrimination.
Les patients sont en droit de recevoir tous les soins de sant
de la reproduction sans discrimination fond
e sur le sexe, le statut marital, le statut sanitaire ou tout autre statut, l
appartenance
un groupe ethnique, la religion, l
ge ou l
habilit
payer.
Benin guarantees access to reproductive healthcare regardless of marital status; therefore, it is placed in the green category for this indicator.
While Benin
s policy environment protects the right of individuals to a full range of methods and to the method of their choice, it falls short of addressing youth access to a full range of contraceptive methods.
For example, the
Loi n
2003-04 du 03 mars 2003 relative
la sant
sexuelle et
la reproduction
states that the full range of legal contraceptives must be authorized and available after consultation as part of an individual
s right to choose from a range of effective and safe contraceptive methods. However, it does not specify that this same right must be extended to youth:
La contraception comprend toute m
thode approuv
e, reconnue effective et sans danger. Elle comprend les m
thodes modernes (temporaires, permanentes), traditionnelles et populaires. Toute la gamme des m
thodes contraceptives l
gales doit
tre autoris
e et disponible apr
s consultation. Le droit de d
terminer le nombre d
enfants et de fixer l
espacement de leur naissance conf
chaque individu la facult
de choisir parmi toute gamme de m
thodes contraceptives effectives et sans danger celle qui lui convient.
The
Strat
gie nationale multisectorielle de sant
sexuelle et de la reproduction des adolescents et jeunes au B
nin, 2010-2020,
which is specifically concerned with youth reproductive health, defines reproductive health as including the right of individuals to the contraceptive methods of their choice, without explicitly stating that youth should be able to access a full range of contraceptive options:
La sant
de la reproduction suppose par cons
quent que les individus aient une vie sexuelle satisfaisante et s
re, ainsi que la capacit
de se reproduire et la libert
de d
cider quand et
quelle fr
quence le faire. Cette derni
re question repose implicitement sur les droits des hommes et des femmes
tre inform
s et
acc
der
des m
thodes de planification familiale (PF) s
res, efficaces, abordables et acceptables qu
ils auront choisies eux-m
mes, ainsi qu
autres m
thodes de leur choix de r
gulation de la f
condit
qui soient conformes
la l
gislation.
The "Plan d
action national budg
de planification familiale du B
nin, 2019- 2023" includes an objective to expand the range of family planning services young people can access to include long-acting reversible methods and postpartum family planning services. However, this activity targets young people living in selected remote areas and does not guarantee their access to a full range of contraceptive methods regardless of age, marital status, or parity.
Because Benin does not have a policy extending access to a full range of methods for youth specifically, it is placed in the yellow category for this indicator. To move to the green category, Benin should clarify that youth can access a full range of methods, including long-acting reversible contraceptives.
Although the availability of emergency contraception (EC) is not factored into the categorization of this indicator, note that Benin
s policy environment does not specifically address youth access to EC.
Benin
s policy environment supports the provision of sexuality education to in-school and out-of-school youth. The
Plan d
action national budg
de planification familiale du B
nin, 2019- 2023
includes a strategy to unify multisectoral efforts intended to strengthen comprehensive sexuality education (CSE) by harmonizing the content of CSE programs currently used in both school and non-school environments, and teaching and providing counseling about family planning services in schools:
Strat
gies
O4. Unifier les efforts multisectoriels (minist
res connexes et autres secteurs) notamment
ducatifs afin d
identifier le gap et exploiter les synergies, assurer l
efficacit
des efforts humains et financiers et renforcer l
ducation compl
la sexualit
A02. Harmoniser le contenu des curricula et mise en
uvre de l
approche d
ducation Compl
la Sexualit
pour les adolescents (e)s et les jeunes scolaris
s, et non/d
scolaris
s ou en situation de vuln
rabilit
en collaboration avec les minist
res charg
s de l
ducation, de l
enseignement sup
rieur, etc. envisageant des visites de centres de sant
accr
s, des s
ances de sensibilisation sur les consultations en PF en milieu scolaire, et l
enseignement potentiel de la PF avant la 3
me.
The
Strat
gie nationale multisectorielle de sant
sexuelle et de la reproduction des adolescents et jeunes au B
nin, 2010-2020
tasks the Ministry of Secondary Education and Technical and Vocational Training with extending SRH education to technical and vocational secondary schools and promoting SRH awareness activities at colleges. The Ministry of Family and National Solidarity is tasked with reaching vulnerable groups of youth with SRH information.
The
Strat
gie nationale multisectorielle
also recognizes the need to tailor information to the specific needs of youth:
Principales options de promotion de la SRAJ [sant
reproductive des adolescents et des jeunes]/VIH/sida :
La prise en compte de l
ge, du genre et des conditions socio-culturelles des adolescents et jeunes dans la d
finition des types et contenus des services d
information, de conseil et de prestations cliniques ou communautaires en SRAJ/VIH/sida.
These policies address two essential components of comprehensive sexuality education (CSE) by personalizing information and reaching across formal and informal sectors and across age groups.
A third component of CSE addressed in Benin
s policy documents is strengthening youth advocacy and civic engagement. The
Strat
gie nationale multisectorielle
places strong emphasis on youth advocacy for adolescent reproductive health information and services:
Les Organisations de jeunesse :
Ces organisations jouent actuellement d
important r
le de mobilisation de jeunes. Elles doivent poursuivre les activit
s de mobilisation des jeunes et adolescents afin d
tre de puissants instruments dans la mise en
uvre de la pr
sente Strat
gie Nationale Multisectorielle. Elles doivent contribuer
la promotion de la CCC [communication pour le changement de comportement] en SRAJ, des prestations de services
base communautaire et le plaidoyer en vue de la mobilisation des leaders communautaires et des partenaires techniques et financiers.
The
Strat
gie nationale multisectorielle
and the
Programme national de sant
de la reproduction, 2011-2015
include a specific objective to strengthen involvement of youth in SRH programming:
Axe : Implication et responsabilisation des jeunes dans la promotion de la SSR [sant
sexuelle et reproductive]/VIH/sida
Objectif sp
cifique :
Renforcer l
implication des structures de jeunes organis
toutes les
tapes du processus de prise de d
cision, de planification, de mise en
uvre et de suivi
valuation.
Although the
Strat
gie nationale multisectorielle
acknowledges gender issues facing youth, such as gender-based violence and forced or early marriages, it does not describe integrating gender into a CSE program.
In addition, the
Plan strat
gique int
de la sant
de la reproduction, de la m
re, du nouveau-n
, de l
enfant, de l
adolescent et jeune (SRMNEAJ), 2017-2021
tasks
the Ministry of Secondary Education and Technical and Vocational Training with integrating SRH education into school curricula for adolescents and youth, training teachers on curriculum content, and organizing community sensitization activities. The "Plan strat
gique int
also tasks the Ministry of Justice with extending SRH education activities for adolescents and youth who are incarcerated.
The
Strat
gie nationale multisectorielle de la sant
sexuelle et de la reproduction des adolescents et jeunes, 2018-2022
introduces Benin's intention to establish a CSE curriculum
in the education system with a goal to eventually scale-up the curriculum to provide it to out-of-school youth:
Interventions
3.6 Instauration d'un programme d
ducation
la sexualit
responsable en milieu scolaire et non scolaire
Activit
s
3.6.1 Accompagner le processus d'int
gration de l'
ducation
la sant
sexuelle dans le syst
ducatif
3.6.2 Assurer le suivi du processus d'int
gration de l'
ducation
la sant
sexuelle dans le syst
ducatif
3.6.3 Rendre disponible les curricula d'
ducation
la sant
sexuelle en milieu extra-scolaire
3.6.4 Pr
parer la mise
chelle du Programme d'
ducation
la sant
sexuelle en milieu extra-scolaire
Benin
s policy environment is supportive of sexuality education but does not reference all nine of the United Nations Population Fund (UNFPA) essential components of CSE. Therefore, Benin is placed in the yellow category for this indicator. Going forward, additional sexuality education policies should consider all nine UNFPA essential components of CSE.
The
Strat
gie nationale multisectorielle de sant
sexuelle et de la reproduction des adolescents et jeunes au B
nin, 2010-2020
and the
Programme national de sant
de la reproduction, 2011-2015
include specific objectives to train providers to offer adolescent-friendly contraceptive services. Additionally, provider training described in the
Plan d
action national budg
de la planification familiale du B
nin, 2019-2023
includes an objective to improve FP services for adolescents and young people by offering capacity-building activities to providers:
Strat
gie
O1. Am
liorer le plateau technique des formations sanitaires pour l
offre de services de PF de qualit
de 2019
2023.
A4. Renforcement des capacit
s des prestataires des formations sanitaires publiques et priv
es pour l
offre de services conviviaux et adaptes de SRAJ [sante de la reproduction des adolescents et des jeunes]
: Renforcer les capacit
s des prestataires de 5% des FS [formations sanitaires] publiques et priv
es (soit 114 FS offrant la PF) par an ans dans le domaine de l
offre des services de PF adaptes aux adolescentes et jeunes permettra de lever l
obstacle lie
attitude de certains prestataires face aux adolescents et jeunes qui se pr
sentent dans les centres de sant
pour adopter les m
thodes de PF. Elle sera r
alis
travers la formation, l
nagement des structures de soins, la supervision et le suivi des prestations.
The
Strat
gie nationale multisectorielle de sant
sexuelle et de la reproduction des adolescents et jeunes au B
nin, 2010-2020
states that a youth-friendly FP service setting should provide confidentiality and affordability:
La formation sanitaire attrayante pour les adolescents et jeunes se d
finit comme un centre d
accueil ou de conseil, une maison des jeunes, offrant un bon accueil, une ambiance de gait
aise, de confidentialit
, une prise en charge ad
quate, un traitement et des produits
moindre co
t.
The "Plan op
rationnel de r
duction de la mortalit
maternelle et n
onatale au B
nin, 2018-2022
identifies improving adolescent
s access to FP through the provision of free contraceptives as a priority
:
Des priorit
s ont
formul
es pour la p
riode 2018
2022 au nombre desquelles figurent :
- La gratuit
de la Planification Familiale favorisant l
s des adolescentes et jeunes
la contraception
Activit
: Offrir gratuitement toutes les gammes de produits contraceptifs dans les formations sanitaires et cabinets priv
s de soins.
The "Plan national de d
veloppement sanitaire, 2018-2022" also includes free access to FP for young people and women of reproductive age as a priority action to reduce morbidity and mortality among adolescents and young people:
5.5.2. Orientation Strat
gique (OS2): Prestation de service et l
lioration de la qualit
des soins
Objectifs Sp
cifiques :
2.1 R
duire la morbidit
, la mortalit
de la m
re, du nouveau n
, de l
enfant, de l
adolescent et du jeune
Axes d
interventions :
2.1.2 Intensification des services de la Planification Familiale
Actions prioritaires:
- Assurer la disponibilit
des produits traceurs de la PF jusqu
au dernier niveau des prestations de services ;
- Renforcer l
rationnalisation du plan d
action budg
de PF ;
- Assurer la gratuit
de l
s des jeunes et des femmes en
ge de procr
la PF.
The
Plan d
action national budg
de planification familiale du B
nin, 2019-2023
includes activities to provide user-friendly family planning services to young people, such as by making contraceptive services free, creating youth-friendly centers, and training providers:
Activit
s
2.1.1 Mettre en place un m
canisme d'exemption des co
ts des contraceptifs pour les adolescents et jeunes
2.1.2 Augmenter
de 50% la couverture nationale
en centres conviviaux int
s pour les adolescents et jeunes
2.1.3 Faciliter l
utilisation des contraceptifs par les adolescentes et jeunes vuln
rables
2.1.4 Elaborer et mettre en
uvre l'initiative
Les formations sanitaires et centres de promotion sociale amis des adolescents et jeunes
Because Benin
s policy documents address all three service-delivery elements of youth-friendly services, Benin is placed in the green category for youth-friendly FP service provision.
The
Strat
gie nationale multisectorielle de sant
sexuelle et de la reproduction des adolescents et jeunes au B
nin, 2010-2020
includes an objective to involve local leaders in information and communication activities:
Objectif sp
cifique N
2 : Renforcer l
implication des Elus locaux, des leaders communautaires et religieux dans les actions d
information sur la
SRAJ [sant
reproductive des adolescents et des jeunes]/VIH/sida chez les adolescents et jeunes.
2.1 Organiser au niveau de chaque commune du pays un atelier d
laboration des plans op
rationnels de communication en SRAJ/IST[infections sexuellement transmissibles]//VIH/sida au profit des
lus locaux et les leaders communautaires et religieux en tenant compte des r
alit
s de chaque commune.
The
Strat
gie nationale multisectorielle
also aims to consider gender when designing reproductive health information and services for youth:
3.2. Principales options de promotion de la SRAJ/VIH/sida
2. La prise en compte de l
ge, du genre et des conditions socio-culturelles des adolescents et jeunes dans la d
finition des types et contenus des services d
information, de conseil et de prestations cliniques ou communautaires en SRAJ/VIH/sida.
3.3 Principes directeurs
La prise en compte des valeurs socioculturelles, de l
thique et du genre dans la programmation des interventions.
Additionally, the
Politique nationale de la jeunesse, 2001
contains a specific objective and corresponding strategy to consider gender as part of the sexual and reproductive health of adolescents:
Objectif Sp
cifique 11 : Contribuer au d
veloppement de la sant
physique, mentale, psychique, sexuelle et de la reproduction des adolescents et des jeunes selon l'approche genre.
Strat
gie 11- 3 : Promotion de la sant
sexuelle et de reproduction des adolescents et jeunes et d'un environnement physique, l
gal et social favorisant l'approche genre.
The
Plan strat
gique int
de la sant
la reproduction, de la m
re, du nouveau-n
, de l
enfant, de l
adolescent et jeune (SRMNEAJ), 2017-2021
tasks the Ministry of Social Affairs and Microfinance with advocacy activities that include promoting dialogue between parents and their child:
Le Minist
re en charge des affaires sociales
:
Il renforcera la promotion du dialogue entre parents et enfants dans le cadre des activit
s de plaidoyer et de formation que d
veloppent les services centraux et d
centralis
s de ce minist
re.
The
Strat
gie nationale multisectorielle de la sant
sexuelle et de la reproduction des adolescents et jeunes, 2018-2022
emphasizes the need to address gender issues in adolescent and youth reproductive health strategies, referencing the "Loi n 2003-04 du 03 mars 2003 relative
la sant
sexuelle et la reproduction," which states the right to reproductive health without discrimination.
The
Plan d
action national budg
de planification familiale du B
nin, 2019-2023
also outlines an objective to achieve a supportive environment for promoting family planning services by mobilizing support from political leaders, religious figures, and local authorities:
Objectif 4 : Garantir un environnement favorable pour la PF
travers :
Le renforcement des activit
s de plaidoyer aupr
s des d
cideurs (Pr
sident de la R
publique du B
nin, Premi
re Dame du B
nin, Institutions nationales, minist
re de la sant
et minist
res connexes) et des leaders administratifs, traditionnels, religieux et des
lus.
These policies outline a detailed strategy to build community support for youth family planning services and to address gender norms, including specific interventions. Therefore, Benin is placed in the green category for this indicator.
The
Politiques et normes en mati
re de sant
de la reproduction au Burkina Faso, 2010
states that access to reversible contraceptive methods should not require spousal consent:
Les femmes et les hommes en
ge de procr
er pourront avoir acc
s aux m
thodes contraceptives r
versibles sans recours au consentement de leur conjoint. Toutefois, l
accent doit
tre mis sur l
importance du dialogue dans le couple pour l
adoption d
une m
thode contraceptive.
However, Burkina Faso
s policies do not adequately address parental consent. Therefore, Burkina Faso is placed in the yellow category for this indicator because its policies address one but not both forms of consent.
While the
Plan strat
gique sant
des adolescents et des jeunes, 2015-2020
describes provider judgment as a barrier to youth access to healthcare, it does not include an explicit statement that providers may not use personal bias or discrimination when offering youth FP services. Therefore, Burkina Faso is placed in the gray category for this indicator.
The
Loi portant sant
de la reproduction, 2005
states that all individuals, including adolescents, have equal rights and dignity in reproductive health throughout their life, regardless of age:
Article 8 : Tous les individus y compris les adolescents et les enfants sont
gaux en droit et en dignit
en mati
re de sant
de la reproduction.
Le droit
la sant
de la reproduction est un droit fondamental garanti
tout
tre humain, tout au long de sa vie, en toute situation et en tout lieu.
Aucun individu ne peut
tre priv
de ce droit dont il b
ficie sans discrimination aucune fond
e sur l'
ge, le sexe, la fortune, la religion, l'ethnie, la situation matrimoniale ou sur toute autre consid
ration.
Because the law guarantees youth access to FP regardless of age, Burkina Faso is placed in the green category for this indicator.
The
Loi portant sant
de la reproduction, 2005
states that all individuals, including adolescents, have equal rights and dignity in reproductive health throughout their life, regardless of marital status:
Article 8 : Tous les individus y compris les adolescents et les enfants sont
gaux en droit et en dignit
en mati
re de sant
de la reproduction.
Le droit
la sant
de la reproduction est un droit fondamental garanti
tout
tre humain, tout au long de sa vie, en toute situation et en tout lieu.
Aucun individu ne peut
tre priv
de ce droit dont il b
ficie sans discrimination aucune fond
e sur l'
ge, le sexe, la fortune, la religion, l'ethnie, la situation matrimoniale ou sur toute autre consid
ration.
Because the law guarantees youth access to reproductive health, including FP, regardless of marital status, Burkina Faso is placed in the green category for this indicator.
The
Loi portant sant
de la reproduction, 2005
states that adolescents have the right to make decisions about their reproductive health (RH) and to obtain information about all methods of contraception:
Article 11 : Tout individu y compris les adolescents et les enfants, tout couple a droit
information,
l'
ducation concernant les avantages, les risques et l'efficacit
de toutes les m
thodes de r
gulation des naissances.
The
Protocoles de sant
de la reproduction, 2009
state that adolescents should have access to all methods regardless of age or marital status:
Les adolescents et jeunes quel que soit leur
ge, leur statut matrimonial doivent avoir acc
toutes les m
thodes contraceptives.
Further, the
Protocoles
include long-acting reversible contraceptives (LARCs) in the list of contraceptives that should be available to youth. Similarly, the
Politique nationale de population du Burkina Faso, 2000
contains an objective to promote use of RH services among adolescents, including a specific aim to provide a full range of methods:
Objectif interm
diaire :
1.1 : Promouvoir une grande utilisation des services de sant
de la reproduction en particulier par les femmes, les jeunes et les adolescents.
Axes strat
giques :
1.1.2. Mise
la disposition de la population de services de sant
de la reproduction de qualit
y compris une gamme compl
te de m
thodes contraceptives s
res, fiables et
un co
t abordable.
The
Plan national d
ration de planification familiale du Burkina Faso, 2017-2020
includes an objective to expand the range of FP methods, including LARCs, to benefit young people:
Objectif 2 : Garantir la couverture en offre de services de PF et l
s aux services de qualit
en renfor
ant la capacit
des prestataires publics, priv
s et communautaires et en ciblant les jeunes ruraux et les zones enclav
es avec l
largissement de la gamme des m
thodes y compris la mise
chelle des MLDAR [m
thodes
longue dur
action r
versibles] et PFPP [planification familiale du post-partum], l
lioration de la prestation aux jeunes.
Therefore, Burkina Faso is placed in the green category for this indicator.
Although the availability of emergency contraception (EC) is not factored into the categorization of this indicator, it is worth noting that the
Protocoles
do not include EC in the list of contraceptives that should be available to youth.
Several policies in Burkina Faso acknowledge the importance of sexuality education and describe plans for improving its implementation. The
Politiques et normes en mati
re de sant
de la reproduction au Burkina Faso, 2010
state that young people have the right to sexuality education:
Les jeunes ont droit
ducation
la vie sexuelle et
la vie familiale.
The
Politique nationale de population du Burkina Faso, 2000
describes plans for family life and sexuality education in formal and informal education settings and for increasing institutional capacity for population education:
1.5.3. Promotion de l
ducation
la vie familiale et l
ducation sexuelle dans les structures d
enseignement formel et non formel.
2.2.1. Accroissement et/ou consolidation des capacit
s institutionnelles en mati
re de formation et d
enseignement en population et d
veloppement aux diff
rents niveaux du syst
ducatif.
The
Troisi
me programme d
action en mati
re de population, 2012-2016
explains that Burkina Faso
s population education program, l
ducation en mati
re de population (EMP), which could not be obtained for this analysis, includes modules on emerging themes such as citizenship, human rights, HIV/AIDS and other sexually transmitted infections, and youth sexual and reproductive health. EMP was introduced in primary and secondary schools in Burkina Faso in the mid-1980s and has since been extended to reach students in informal settings. The
Troisi
me programme d
action
includes a specific objective to increase the effectiveness of population and citizenship education in formal and informal settings:
Objectif sp
cifique 3 : Rendre effective l
ducation en mati
re de population et de citoyennet
(EmPC) dans 100% des structures du syst
me formel et 95% des structures non formelles.
Similarly, the
Plan national de relance de la planification familiale, 2013-2015
includes an activity to revitalize population education in both formal and informal education settings, including training school nurses and staff at youth centers in a youth-focused approach. The
Plan strat
gique sant
des adolescents et des jeunes, 2015-2020
has a general activity to introduce sexuality education into education and training settings. Furthermore, the
Plan national d
ration de planification familiale du Burkina Faso, 2017-2020
includes priority actions to incorporate modules on comprehensive sexuality education (CSE) in teaching curricula, build the capacity of students and teachers on CSE, and implement a CSE approach for out-of-school young people.
Burkina Faso
s policy environment is promising because it supports the provision of sexuality education and includes some of the essential components of CSE within its sexuality education program, such as reaching youth across formal and informal sectors, human rights, and citizenship. However, all nine components of CSE are not mentioned as part of the CSE program. Therefore, Burkina Faso is placed in the yellow category for this indicator. Future plans for revitalizing sexuality education in Burkina Faso should consider including all nine of the United Nations Population Fund
s (UNFPA
s) essential components of CSE.
The
Plan strat
gique sant
des adolescents et des jeunes, 2015-2020
describes provider judgment and lack of confidentiality as barriers to youth access to health care:
L
offre de SSR [sant
sexuelle et reproductive] de qualit
se trouve limiter par
insuffisance de comp
tences du personnel de sant
. En effet, les
ments suivants participent
entraver la qualit
des soins et des services pour les adolescents et les jeunes : attitude des prestataires non respectueuse et de jugement, droit
la confidentialit
non respect
The
Plan strat
gique
then includes an adjoining aim to train and supervise providers in the provision of youth sexual and reproductive health services:
Axe 2 :
Renforcement de l
offre de soins et des services de SRAJ [sant
reproductive des adolescents et des jeunes] de qualit
Formation continue des prestataires au niveau des formations sanitaires
Renforcement de la supervision des prestataires
Additionally, the
Directives nationales sur la sant
scolaire et universitaire au Burkina Faso, 2008
assert that youth centers in schools and universities should provide affordable contraceptives for students and emphasize the importance of confidentiality when providing services to youth:
II. LES DIFFERENTES INTERVENTIONS NECESSAIRES POUR ASSURER LA PRISE EN CHARGE MEDICO-SOCIALE DES PROBLEMES DE SANTE SCOLAIRE ET UNIVERSITAIRE
2.2.8. Confidentialit
La confidentialit
constitue la pierre angulaire de la fr
quentation de tout service de sant
par les jeunes. Ainsi la confidentialit
ne doit pas
tre n
glig
e par les prestataires parce qu
ils ont affaire
un public souvent plus jeune.
-La confidentialit
doit transpara
tre dans tous les services de sant
. Elle doit en tout temps pr
valoir entre le prestataire et les scolaires et universitaires,
-Les informations concernant un scolaire ou universitaire ne peuvent
tre divulgu
des tiers sauf en cas d
urgence et dans son int
t,
-Les dossiers des scolaires et universitaires doivent
tre gard
s en lieu s
r. Seuls les prestataires peuvent pouvoir y acc
der.
The
Politique et normes en mati
re de sant
de la reproduction, 2010
outlines quality standards for reproductive health. The list of service standards includes patient confidentiality, but is not specific to adolescents and youth:
1.6
Normes de qualit
de services
Pour que les programmes de sant
soient des programmes de qualit
:
- Les services doivent
tre personnalises,
- Les clients doivent
tre traites avec dignit
,
- Les clients doivent
tre trait
s de mani
re confidentielle,
- Les clients ne doivent pas attendre longtemps avant d
tre re
us,
- Les prestataires de service doivent informer les clients sur les m
thodes et services disponibles,
- Les prestataires de sante doivent pouvoir reconnaitre leurs limites.
The
Decret n
2019-0040/PRES/PM/MS/MFSNF/MFPTPS/MATD/MINEFID portant gratuit
des soins et des services de planification familiale au Burkina Faso,
agreed upon in December 2018 by the Council of Ministers, granted free family planning health care to everyone in the country:
Article 1: Il est institu
la gratuit
des soins et des services de planification familiale sur toute l
tendue du territoire national.
Article 2 : La gratuit
de la planification familiale est mise en
uvre dans toutes les formations sanitaires publiques par les agents de sant
base communautaire (ASBC) et au sein des formations sanitaires priv
es conventionn
es du Burkina Faso.
The decree notes that family planning will be free in public and select private facilities in contract with the government, but implementation is voluntary. When the decree was initially announced, the Council of Ministers noted that this policy change would especially benefit adolescents and youth:
L
adoption de ce d
cret permet la mise en
uvre de la mesure de gratuit
de la planification familiale dans les structures de sant
publique de notre pays et une intensification de l
offre des services de la planification familiale au profit des populations notamment les adolescents, les jeunes et les populations vivant en milieu rural.
Burkina Faso has a strong policy environment for the provision of youth-friendly FP services and is accordingly placed in the green category for this indicator.
Burkina Faso
s policies support an enabling social environment for youth-friendly service provision through addressing gender norms and building support in communities.
For example, the
Politiques et normes en mati
re de sant
de la reproduction au Burkina Faso, 2010
acknowledge the multisectoral nature of reproductive health and the required collaboration around gender-related issues, such as:
- la promotion de la scolarisation des jeunes filles et de l
alphab
tisation des femmes,
- la promotion de l
autonomisation financi
re des femmes,
- la promotion d
un environnement physique, politique, juridique, social et
conomique favorable
la sant
, dans un esprit d
quit
entre les sexes.
The
Document de la politique nationale genre du Burkina Faso, 2009" includes an objective to eliminate sociocultural barriers related to health access, including taboos surrounding women accessing reproductive health services:
Objectif 2
. De m
me, en mati
re de sant
, il importe de travailler
liminer certains tabous persistants et
promouvoir la libert
de fr
quentation des services de sant
par les femmes. En outre, l
galit
en mati
re de sexualit
doit
tre promue
travers les programmes de Sant
de la Reproduction et de lutte contre le SIDA.
Several other policy documents from Burkina Faso consider gender-related challenges as they outline support for the promotion of reproductive health services, especially for adolescents and young people.
The "Plan strat
gique sant
des adolescents et des jeunes, 2015-020" includes a priority activity to promote a favorable social environment for adolescent and youth health, including building capacity among adolescent and youth reproductive health community actors on gender issues:
Axe 6 : Promotion d
un environnement social et juridique favorable
la sant
des adolescents et des jeunes
| Actions prioritaires |
Description |
| ...
Renforcement des capacit
s des acteurs de la SRAJ sur les questions de genre et droits humains |
- Identification des besoins
- Orientations sur les questions genre et droits humains
- Sessions de formation
- Suivi et
valuation
|
The
Plan strat
gique sant
des adolescents et des jeunes, 2015-2020
describes specific activities to promote a social environment conducive to the health of adolescents and to reach community leaders and parents about youth sexual and reproductive health:
Axe 6 : Promotion d
un environnement social et juridique favorable
la sant
des adolescents et des jeunes
Renforcement du dialogue parents enfants dans l
ducation sexuelle et les bonnes habitudes d
hygi
ne et de vie des adolescents et des jeunes
- Formation
la vie familiale des parents et des adolescents et des jeunes
- Communication m
dia sur le r
le des parents
- Utilisation des NTIC [nouvelles technologies de l'information et de la communication] pour rappeler le r
le attendu des parents (SMS)
- Communication m
dia sur l
ducation sexuelle, les bonnes habitudes d
hygi
ne et de vie
Implication des leaders communautaires et religieux dans l
ducation sexuelle et les bonnes habitudes d
hygi
ne et de vie des adolescents et jeunes
- Plaidoyer
- Communication m
dia sur l
ducation sexuelle et les bonnes habitudes d
hygi
ne et de vie
Burkina Faso outlines a detailed strategy to build community support for youth FP services and to address gender norms. Therefore, it is placed in the green category for this indicator.
The
Normes des services de sant
de la reproduction, 2012
state that any person of childbearing age can access contraceptives without spousal consent:
Les femmes et les hommes en
ge de procr
er doivent avoir acc
s aux m
thodes contraceptives r
versibles sans recours au consentement de leur conjoint. Toutefois, l
accent doit
tre mis sur l
importance du dialogue dans le couple pour l
adoption d
une m
thode contraceptive.
Although the
Normes des services
address spousal consent, no reviewed policy documents address parental consent. Burundi is placed in the yellow category for this indicator because its policies do not explicitly support youth access to FP services without consent from parents.
The
Normes des services de sant
de la reproduction, 2012
acknowledge youth and adolescent rights to dignity and to receiving FP services from trained professionals:
III.2.3.1. Droits en Sant
Sexuelle et Reproductive
De fa
on sp
cifique, les adolescents et les jeunes jouissent des droits suivants :
- Le droit
la dignit
tre trait
(e) avec courtoisie, consid
ration et pr
venance.
- Le droit de b
ficier d
explications suffisantes de l
intervention que vous subissez lorsque vous recevez des soins de sant
.
- Le droit d
tre pris en charge par des gens form
s et qui ma
trisent ce qu
ils
The "Normes des services" establish service quality standards and note that successful programs require well-trained staff that employ sensitivity toward clients and use clinical judgment:
Des programmes r
ussis exigent un personnel bien form
qui d
montre :
- Attention, sensibilit
et empathie lorsqu
il informe le client,
- Connaissances, attitudes et comp
tences pour fournir les services de SR [sant
reproductive],
- Connaissance des probl
mes r
els ou potentiels et capacit
de les reconna
tre,
- Capacit
de prendre des mesures cliniques appropri
es en r
ponse
ces probl
mes, y compris quand et o
rer les clients qui ont des probl
mes graves ; bon jugement clinique,
While Burundi
s policies acknowledge young people
s right to be treated with dignity and that successful facilities show empathy and exercise clinical judgment, they fail to explicitly require health workers to provide medically advised FP services to youth without personal bias or discrimination. Burundi is placed in the gray category for this indicator.
The
Politique nationale de sant
, 2016-2025" prioritizes access to sexual and reproductive health (SRH) services for adolescents and young people to improve maternal, newborn, and adolescent health:
P
riode de l
adolescence (10- 20 ans) : (1) l
information et l
offre des services de sant
sexuelle et reproductive des adolescent(e)s et des jeunes ax
e sur la pr
vention des grossesses pr
coces, la pr
vention des IST[infections sexuellement transmissibles]-VIH/SIDA, la pr
vention des mariages pr
coces
P
riode de la jeunesse (20- 24 ans) : (1) l
information et l
offre des services de sant
sexuelle et reproductive des jeunes ax
e sur la pr
vention des grossesses pr
coces, la pr
vention des mariages et maternit
coces, la pr
vention des IST-VIH/SIDA
The "Loi n
1/012 du 30 mai 2018 portant code de l
offre des soins et services de sant
au Burundi
supports access to health without discrimination based on age:
Chapitre II : Des principes directeurs de la politique nationale de sant
. Nul ne peut
tre l'objet de discrimination du fait notamment de son origine, de sa race, de son ethnie, de son sexe, de sa couleur, de sa langue, de sa situation sociale, de ses convictions religieuses, philosophiques, ou politiques, du fait d
un handicap physique ou mental, du fait d
tre porteur du VIH/Sida ou de toute autre maladie incurable.
The
Module de formation des prestataires de soins en sant
sexuelle et reproductive des adolescents et des jeunes, 2020
notes this access to health services includes SRH and FP:
Les adolescents et les jeunes ont les m
mes droits en SSR [sant
sexuelle et reproductive] que les adultes, ils sont encourag
exprimer leurs besoins pour de plus amples informations et un meilleur acc
s aux services
The
Normes des services de sant
de la reproduction, 2012
affirm the rights that adolescents and young people enjoy, including the right of access to SRH services and free choice of contraceptive methods:
III.2.3.1. Droits en Sant
Sexuelle et Reproductive
De fa
on sp
cifique, les adolescents et les jeunes jouissent des droits suivants :
- Le droit
information :
tre inform
(e) des avantages et de la disponibilit
de l
ensemble des services essentiels.
- Le droit d
s : obtenir l
ensemble des services de SSR et
un prix abordable sans discrimination de sexe, de croyances, de race, d
ethnie, de statut marital ou d
origine g
ographique.
- Le droit de libre choix : d
cider librement de l
utilisation des services de planification familiale et de la m
thode
utiliser ou de l
utilisation de l
un des quelconques services disponibles.
As Burundi
s policies support youth access to family planning regardless of age, Burundi is placed in the green category for this indicator.
The "Normes des services de sant
de la reproduction, 2012," which include family planning in a service package for youth, support adolescent and youth access to sexual and reproductive health services without discrimination based on marital status:
III.2.3.1. Droits en Sant
Sexuelle et Reproductive
De fa
on sp
cifique, les adolescents et les jeunes jouissent des droits suivants :
...
Le droit d
s : obtenir l
ensemble des services de SSR [sant
sexuelle et reproductive] et
un prix abordable sans discrimination de sexe, de croyances, de race, d
ethnie, de statut marital ou d
origine g
ographique.
Le droit de libre choix : d
cider librement de l
utilisation des services de planification familiale et de la m
thode
utiliser ou de l
utilisation de l
un des quelconques services disponibles.
Because the law supports youth access to FP services regardless of marital status, Burundi is placed in the green category for this indicator.
The "Politique nationale de la sant
de la reproduction, 2007
aims to improve the availability and accessibility of FP services by expanding contraceptive method options, including long-acting reversible contraceptives (LARCs), without specifically mentioning youth access:
Am
lioration de la disponibilit
et de l
accessibilit
des services de PF de qualit
:
- Etendre la distribution
base communautaire des contraceptifs non prescriptibles au niveau national ;
- Elargir la gamme des m
thodes contraceptives en mettant l
accent sur les m
thodes de longue dur
action.
The
Politique nationale de sant
, 2016-2025" describes the need to allow informed free choice of contraceptives to reach contraceptive coverage goals:
Le renforcement de l
s et l
utilisation des services de planification familiale de qualit
tenant compte des besoins et du choix libre
clair
de l
individu afin d
atteindre une couverture contraceptive d
au moins 50 %.
Burundi's
Normes des services de sant
de la reproduction, 2012
note that a range of contraceptive methods must be available at all levels of health care:
Toutes les m
thodes de contraception suivantes doivent
tre disponibles selon les normes de paquets d
activit
finies par niveaux de soins :
- La m
thode de l
allaitement maternel avec am
norrh
e (MAMA)
- Les spermicides
- Les pr
servatifs masculins et f
minins
- Les pilules
- Les injectables
- Les implants
- Le Dispositif intra-ut
rin (DIU)
- La Contraception Chirurgicale Volontaire (CCV)
- La m
thode naturelle
While the
Normes des services
further note that men and women of reproductive age have access to all reversible contraceptive methods without spousal consent and that adolescents and youth have the right to freely decide on which methods to use, they do not reference parity or marital status.
Although policy documents value method choice and mix, future policy documents should clearly state that a full range of methods, including LARCs, are available for youth regardless of age, marital status, and parity. Burundi is placed in the yellow category for this indicator.
Although the availability of emergency contraception (EC) is not factored into the categorization of this indicator, it is worth noting that the reviewed policies do not address youth access to EC.
The
Politique nationale de sant
, 2016-2025" aims to introduce sex education and the promotion of gender equality into school curricula, yet only references young people ages 20 to 24:
L
s pour les jeunes de 20- 24 ans
(1) l
information et l
offre des services de sant
sexuelle et reproductive des jeunes ax
e sur la pr
vention des grossesses pr
coces, la pr
vention des mariages et maternit
coces, la pr
vention des IST[infections sexuellement transmissibles]-VIH/SIDA, (2) services de pr
vention et prise en charge des addictions (alcool, tabac, drogues), (3) l
ducation nutritionnelle des jeunes et (4) dans le cadre de l
intersectorialit
, introduire des s
ances d
ducation sexuelle et promotion de l
galit
du genre.
The
Politique nationale" includes the introduction of sexuality education adapted to adolescents and young people
s needs in school curricula:
P
riode de l
adolescence (10- 20 ans) :
Dans le cadre de l
intersectorialit
: - introduction de l
ducation sexuelle adapt
e aux adolescent(e)s et aux jeunes dans le cursus scolaire, - promotion de l
galit
du genre dans les
coles,
P
riode de la jeunesse (20- 24 ans)
Dans le cadre de l
intersectorialit
: - introduction de l
ducation sexuelle adapt
e aux jeunes dans le cursus scolaire et promotion de l
galit
du genre, - protection des jeunes contre les violences sexuelles et autres formes de violences bas
es sur le Genre.
The "Plan d
ration de la planification familiale, 2015-2020" describes activities to ensure sexual and reproductive health information reaches adolescents and young people in and out of school:
Strat
gie DE3 : Initiation de strat
gies novatrices de communication en direction des adolescents et des jeunes scolaris
s et non scolaris
s. Au niveau de cette strat
gie, il sera question d'utiliser les espaces et les outils de communication auxquels sont beaucoup attach
s les adolescents et les jeunes pour les sensibiliser sur la PF.
...
Activit
DE3.2 : Appuyer l'int
gration de l'
ducation sexuelle compl
te dans les programmes scolaires non encore couverts (8
me, 7
me, 6
me, 5
me) en synergie avec le minist
re en charge de l
ducation. Il sera question d'aider
ce qu'il soit pris en compte dans les curricula de formation des classes de la (8
me, 7
me, 6
me, 5
me) l'
ducation sexuelle. Il s'agira surtout d'aider
la confession et
la distribution des diff
rents manuels.
Activit
DE3.3 : Mettre en
uvre/utiliser les outils de formation sur la SSRAJ [sant
sexuelle et reproductive des adolescents et des jeunes] au niveau communautaire avec tous les acteurs (
coles, centres jeunes, associations de jeunes) dans l'ensemble des provinces du pays. Cette activit
consistera
reproduire et
mettre
la disposition de tous les acteurs au niveau communautaire et ce dans les 17 provinces du pays, les outils de formation sur la SSRAJ. Ces outils serviront de base de formation dans les diff
rents centres de regroupement des jeunes.
However, as part of a strategic goal to reduce sexually transmitted infections, undesired pregnancies, and high-risk abortions in adolescents and young people, the
Politique nationale de la sant
de la reproduction, 2007
aims to promote both abstinence and contraceptive use:
- Promouvoir l
abstinence et /ou l
usage correcte et syst
matique du Pr
servatif ;
- Promouvoir la contraception chez les jeunes et les adolescents ;
Burundi
s policy environment is promising as it mandates sexuality education as a necessity for increasing contraceptive use. However, existing activities for implementation do not include each of the United Nations Population Fund
s (UNFPA
s) nine elements of comprehensive sexuality education. Therefore, Burundi is placed in the yellow category for this indicator.
Multiple policy documents outline young people
s rights when seeking sexual and reproductive health (SRH) services. The
Normes des services de sant
de la reproduction, 2012
outline adolescents
and youth rights when seeking SRH services, including the right to privacy, confidentiality, trained providers, and access to services at an affordable price:
III.2.3. Sant
des Jeunes
III.2.3.1. Droits en Sant
Sexuelle et Reproductive De fa
on sp
cifique, les adolescents et les jeunes jouissent des droits suivants :
- Le droit d
s : obtenir l
ensemble des services de SSR [sant
sexuelle et reproductive] et
un prix abordable sans discrimination de sexe, de croyances, de race, d
ethnie, de statut marital ou d
origine g
ographique.
- Le droit
intimit
: b
ficier d
un environnement intime durant l
assistance ou la prestation des services.
- Le droit
la dignit
tre trait
(e) avec courtoisie, consid
ration et pr
venance.
- Le droit
la confidentialit
tre assur
(e) que toute information personnelle restera confidentielle.
The
Loi n
1/012 du 30 mai 2018 portant code de l
offre des soins et services de sant
au Burundi" also guarantees all patients the right to the confidentiality of their information:
Article 16
: Tout patient a le droit de d
cider de l'usage des informations m
dicales le concernant et les concernant et les conditions dans lesquelles elles peuvent
tre transmises
des tiers. Les
tablissements de sant
doivent garantir la confidentialit
des informations qu
ils d
tiennent sur leurs patients m
me apr
s leur d
s. Toutefois le secret m
dical n'est pas opposable au patient. Le respect du secret m
dical peut
tre
carte dans les cas pr
vus par la loi.
The
Directives de mise en place et de fonctionnement d
un centre de sant
ami des jeunes, 2014
outline the characteristics of health centers that provide youth-friendly SRH services. The
Directives
emphasize equitable access to services, respect for confidentiality, affordable services, and avoiding stigma and judgment:
IV- 4 Caract
ristiques des services offerts dans un CDS [centre de sant
] ami des jeunes
Les services de sant
sexuelle et reproductive adapt
s aux jeunes et adolescents de qualit
sont :
-
quitables pour tous les jeunes et adolescents sans distinction de sexe, de religion, de niveau d
tude, d
ethnie ou toute autre appartenance sociale;
- Efficaces et rapides, offert avec ou sans rendez-vous parce qu'ils r
pondent aux besoins des jeunes et sont appr
s par eux.
- Dispens
s par des prestataires form
s et comp
tents
: form
sur des outils harmonis
s portant sur la SSRAJ, la psychologie de l
adolescent et la communication adapt
e aux jeunes etc
; personnel compr
hensif, accueillant, pr
venant, qui ne jugent pas et qui traitent chaque adolescent avec autant de soins et de respect. Un personnel avis
y compris le personnel d
appui, motiv
et bien soutenu (supervis
par les Equipes Cadres de District sanitaire)
- Efficients parce qu'ils ne gaspillent pas les ressources ;
- Accessibles et abordables
- Confidentiels et garantissant le respect de l
anonymat et
vitant la stigmatisation et le jugement.
De nature
fournir des informations sur base des documents p
dagogiques int
(le plus de services possibles et au m
me moment)
des heures favorables
la disponibilit
des jeunes en l
occurrence les apr
s-midi et les week end.
The "Politique nationale de la sant
de la reproduction, 2007" aims to build the capacity of providers to communicate with young people:
Renforcer les capacit
s des prestataires de sant
et autres intervenants en
Comment communiquer efficacement avec les jeunes et les adolescents.
As part of a strategic goal to reduce sexually transmitted infections, undesired pregnancies, and high-risk abortions in adolescents and young people, the
Politique nationale
plans to integrate adolescent and youth health into the minimum package of services for in-service training and promote user-friendly reproductive health services.
The "Plan d
ration de la planification familiale, 2015-2020" includes a strategic priority to improve the supply of FP services, including ensuring adolescents and young people access services adapted to their needs. The priority intervention includes multiple activities to train health care workers or integrate FP into service curricula:
Activit
O1.1 :
tendre l'offre de services de PF dans l'ensemble des CDS et h
pitaux publics
Rendre disponible les services de PF dans une structures, il s'agira essentiellement de former au moins deux prestataires, d'
quiper les structures en mat
riel de communication pour le changement de comportement, en mat
riel de pr
vention des infections, mat
riel de pose et retrait de DIU [dispositif intra-ut
rin] et d'implant puis d'approvisionner les FOSA [formations sanitaires] en produits contraceptifs de qualit
.
...
Activit
O1.3: Int
grer l'offre de PF dans les services de sant
de toutes les entreprises qui en disposent
Il s'agira essentiellement de faire des plaidoyers, de former et d'
quiper les services de sant
de ces entreprises
offrir des services de PF de qualit
.
...
Activit
O1.7 :Passer
l'
chelle l'int
gration de la PF dans le paquet d
activit
de tous les Agents de Sant
Communautaire (ASC) du pays
The
Plan d
ration
also includes 10 more activities to build the capacity of service providers to give quality FP services, including modern contraceptives, although the activities are not specific to youth. The activities also involve on-the-job training and the integration of modules into in-service training. Finally, the
Plan d
ration
lists two specific activities to strengthen access to youth-friendly FP services, including equipping spaces and training providers:
Strat
gie O3 : Renforcement de l'acc
s des adolescents et jeunes aux services adapt
leurs besoins Cette strat
gie a pour objectif de faciliter davantage l'acc
s des services de PF aux adolescents et aux jeunes. Elle comprend 2 activit
s.
Activit
O3.1 : Am
nager et
quiper deux CDS par district pour l'int
gration effective de l'offre de services conviviaux pour adolescents et aux jeunes Il s'agira d'am
nager et d'
quiper des espaces
l'int
rieur des CDS qui soit adapt
s aux adolescents et aux jeunes. Ce qui facilitera l'offre des services de PF
ces derniers. 73 CDS seront am
s et
quip
s pour offrir des services adapt
s aux adolescents et aux jeunes pour r
pondre
un besoin de 90 CDS exprim
par le pays.
Activit
O3.2 : Former les prestataires de deux CDS par district pour l'offre de services conviviaux pour adolescents et aux jeunes Des sessions de formation seront organis
es pour former des prestataires
l'offre des services de PF adapt
aux besoins des jeunes. Cette activit
permettra de renforcer les capacit
s de 146 prestataires.
The "Module de formation des prestataires de soins en sant
sexuelle et reproductive des adolescents et des jeunes, 2020," which provides the curriculum for training providers on adolescent and youth SRH, notes that providers should be providing evidence-based services without judgment to help adolescents and youth develop autonomy over their sexual health:
CHAPITRE IV : LES DROITS DES ADOLESCENTS ET DE JEUNES EN SANTE SEXUELLE ET REPRODUCTIVE
Les adolescents et les jeunes ne comprennent pas toujours enti
rement leurs droits sexuels ou il se peut qu
ils ne sachent m
me pas qu
ils ont des droits. En tant que prestataires, le fait de savoir offrir des informations compl
tes et factuelles sans jugements, peut aider les adolescents et les jeunes
comprendre leurs options et peut les aider
acqu
rir suffisamment d
autonomie pour prendre en charge leur sant
sexuelle.
CHAPITRE XIII : CLARIFICATION DES VALEURS ET ATTITUDES DESPRESTATAIRES A PROPOS DE LA SEXUALITE DES ADOLESCENTS ET DES JEUNES
D
clarez que la prochaine s
ance fournira aux participants des renseignements qui d
montreront l
importance de la prestation de services de SSR aux adolescents et aux jeunes sans jugement de valeur.
The "Plan strat
gique national de la sant
de la reproduction, maternelle, n
onatale, infantile et des adolescents, 2019-2023" details the priority intervention to improve the availability, accessibility, and use of adolescent health care and services, including reproductive health. The activities outlined discuss the need to improve the youth-friendly services environment but fall short of mentioning privacy and confidentiality.
The policies reviewed clearly address the need to train and support providers to offer adolescent-friendly contraceptive services. However, while Burundi
s policy environment addresses adapting youth-friendly spaces and free and subsidized SRH services, it fails to link them directly to youth family planning services. Burundi is placed in the yellow category for this indicator.
The
Politique nationale de la sant
de la reproduction, 2007
plans to strengthen advocacy within the community for increased support of youth FP:
Renforcement du plaidoyer aupr
s des pouvoirs publics pour un engagement plus accru en faveur de la PF :
Mener un plaidoyer vigoureux aupr
s de tous les intervenants existants (d
cideurs politiques, leaders communautaires et religieux) et potentiels en faveur d
une meilleure prise de conscience de la probl
matique de la PF et de la promotion de l
ralis
aux services de PF par les femmes, les hommes et les jeunes
The
Plan d
ration de la planification familiale, 2015-2020
outlines strategies and activities to create an environment favorable to FP:
Strat
gie DE1 : Mobilisation sociale pour l'utilisation de la PF
Cette strat
gie vise
promouvoir la PF aupr
s des populations en g
ral et des femmes, des adolescents et des jeunes puis des leaders communautaires.
Activit
DE1.1 : Elaborer des supports de sensibilisation de la population bas
s sur les facteurs explicatifs de la faible utilisation de la PF et adapt
chaque cible
Activit
DE1.2 : Organiser des sensibilisations cibl
es de la population
partir des facteurs explicatifs de la faible utilisation de la PF
Activit
DE1.3 : Organiser des rencontres d'
changes et de plaidoyer avec les leaders communautaires (religieux, leaders d
opinion) pour leur implication en faveur de la PF
...
Activit
DE1.7 : Organiser des activit
s de mobilisation communautaire (concours, jeux, chansons, sketchs) pour la promotion de la PF. Cette activit
va consister
organiser des journ
es culturelles et r
atives dans chacune des 17 provinces du pays. Il s'agira de cr
er des regroupements attractifs de masse en vue de faire la promotion de la PF
travers des jeux concours, cin
mobiles, chansons, sketchs...
The "Plan d
ration" also includes promoting male engagement in FP as a priority and describes activities to use male champions and integrate FP activities into male community groups:
Strat
gie DE2 : Promotion de l
engagement des hommes en PF Cette strat
gie vise
faire
amener les hommes
s'impliquer d'avantage dans la promotion et
la pratique de la PF.
Activit
DE2.1 : Utiliser les hommes champions pour la promotion de la PF aupr
s de leurs pairs Il s'agira d'identifier dans les diff
rentes communaut
s et de former des champions ou des personnes qui se sont engag
dans la pratique la PF. Ces champions feront ensuite la promotion de la PF en partageant leurs exp
riences aupr
s de leurs pairs dans les lieux de rencontre privil
s par les hommes.
Activit
DE2.2 : Produire et diffuser des outils de communication en faveur de la PF ciblant les hommes. Des messages seront con
us sp
cifiquement pour hommes en mettant l'accent les aspects qui poussent les hommes
constituer un obstacle
la promotion et
la pratique de la PF.
Activit
DE2.3 : Int
grer les activit
s de PF dans les programmes des groupements communautaires des hommes (p
cheurs, agriculteurs, motards, militaires...) en utilisant des messages adapt
s aux diff
rents milieux. Il sera ici question d'organiser des sessions de formation et d'
changes
l'endroit des membres des diff
rents groupements des hommes (p
cheurs, d'agriculteurs, motards, militaires...) pour permettre
ces derniers de sensibiliser leurs pairs sur la PF au cours de leurs activit
s.
Burundi
Directives de mise en place et de fonctionnement d
un centre de sant
ami des jeunes, 2014
and the
Module de formation des prestataires de soins en sant
sexuelle et reproductive des adolescents et des jeunes, 2020
also acknowledge the importance of involving parents, community and religious leaders, and local administration representatives to create a more enabling environment for youth and adolescent sexual and reproductive health.
Burundi
s policies outline specific interventions to build support within the larger community for youth FP and address gender and social norms. Burundi is therefore placed in the green category for this indicator.
Cameroon is placed in the gray category for this indicator because its policies do not support youth access to FP services without consent from parents and spouses.
The "Plan strat
gique national de la sant
des adolescents et des jeunes au Cameroun, 2015-2019" acknowledges that provider bias toward young people prevents them from accessing services:
Les services, notamment de planning familial, sont inaccessibles aux jeunes. Ils rencontrent beaucoup de barri
res : culturelles,
conomiques, l
attitude discriminatoire des prestataires de services.
The "Normes et standards en SR-PF au Cameroun, 2018" state in the norms on counseling that providers should not force clients to adopt any method:
Si le client se d
cide, le counseling l
aide
choisir une m
thode de contraception appropri
e, l
aide
comprendre comment l
utiliser, et le rend capable de l
utiliser correctement pour une protection s
re et efficace. Cette information doit permettre une bonne compr
hension de l'efficacit
des m
thodes contraceptives. Elle doit permettre au client de bien comprendre comment les utiliser correctement, de quelle mani
re elles agissent, quels en sont les effets secondaires courants, quels sont les risques et les avantages pour la sant
, quels sont les signes et sympt
mes n
cessitant de revenir consulter, des informations sur le retour
la f
condit
apr
s arr
t des m
thodes et des informations sur la pr
vention des IST [infections sexuellement transmissibles]. Les prestataires ne doivent pas imposer
un client l'adoption d'une quelconque m
thode.
Cameroon
s policies, however, do not explicitly state that providers must refrain from applying their personal biases and beliefs when providing FP services to youth. Therefore, Cameroon falls into the gray category for this indicator.
The
Protocoles et algorithmes en SR-PF au Cameroun, 2017" state that adolescents should have access to FP methods of their choosing:
En ce qui concerne la planification familiale, les adolescents peuvent utiliser n
importe quelle m
thode de contraception et doivent avoir acc
un choix
tendu. L
ge ne constitue pas
lui seul une raison m
dicale permettant de refuser une m
thode a un adolescent.
Cameroon is placed in the green category for this indicator because the policy environment confirms that youth must be permitted access to FP services regardless of age.
The
Protocoles et algorithmes en SR-PF au Cameroun, 2017" support youth
s need for FP services regardless of marital status:
Les adolescentes sexuellement actives mari
es ou non ont des besoins en mati
re de planification familiale. Il faut
viter que le cout des services et des m
thodes ne limitent pas les possibilit
s de choix.
In addition, the
Normes et standards en SR-PF au Cameroun, 2018
state that clients have the right to access reproductive health services regardless of their family situation:
2.1.2. Droit
s aux services
Le droit
s aux services de [sant
reproductive] stipule que:
...
Les clients doivent recevoir les services quel que soit leur sexe, leur principe, leur couleur, leur situation familiale, leur orientation sexuelle ou leur r
sidence.
Although the need for family planning among unmarried adolescents is recognized, the
Normes et standards
do not provide enough language affirming the rights of unmarried youth to access these services. Since Cameroon
s policies lack specific language supporting the right of unmarried people to FP services, it is placed in the gray category for this indicator.
The
Plan strat
gique national de la sant
des adolescents et des jeunes au Cameroun, 2015-2019
aims to reduce morbidity and mortality linked to reproductive health in adolescents and young people through increased prevalence of modern FP methods:
Augmenter le taux de pr
valence contraceptive (m
thodes modernes) chez les adolescentes et les jeunes filles d
ici 2019 ;
The
Protocoles et algorithmes en SR-PF au Cameroun, 2017" state that adolescents should have access to FP methods of their choosing:
En ce qui concerne la planification familiale, les adolescents peuvent utiliser n
importe quelle m
thode de contraception et doivent avoir acc
un choix
tendu. L
ge ne constitue pas
lui seul une raison m
dicale permettant de refuser une m
thode a un adolescent.
...
Les adolescentes sexuellement actives mari
es ou non ont des besoins en mati
re de planification familiale. Il faut
viter que le co
des services et des m
thodes ne limitent pas les possibilit
s de choix.
The "Protocoles et algorithmes" also provide a copy of a rapid consultation checklist from the World Health Organization
s eligibility criteria for contraceptive use (2015), as well as a detailed explanation of each contraceptive method and its definition, eligibility criteria, advantages, disadvantages, and usage. While there is specific reference to youth eligibility and access to a range of methods, the policies do not include long-acting reversible contraceptives.
The
Normes et standards en SR-PF au Cameroun, 2018
state that the full range of contraceptives must be authorized after consultation as part of an individual
s right to choose from a range of methods. However, it does not specify that this same right must be extended to youth:
2.1.3. Droit au choix du service
Le droit du client(e) au choix des services de SR [sant
reproductive] stipule que :
- Chaque individu d
cide librement de pratiquer la planification familiale ou non.
- Chaque individu d
cide librement de sa m
thode contraceptive.
- Les prestataires de services doivent pr
senter
tout client(e) la gamme compl
te de m
thodes contraceptives pour lui permettre de faire son choix...
- Une cliente qui a choisi une m
thode
laquelle elle n'est pas
ligible, doit en
tre inform
e et les m
thodes alternatives devront lui
tre offertes.
While Cameroon
s policy environment protects the right of individuals to choose from a full range of methods, it falls short of including explicit language allowing youth to access to a full range of contraceptive methods, including long-acting reversible contraceptives. Cameroon is placed in the yellow category for this indicator.
Although the availability of emergency contraception (EC) is not factored into the categorization of this indicator, it is worth noting that the
Protocoles et algorithmes
include EC in the list of contraceptives available for clients, with no mention of youth eligibility.
Cameroon
s policy environment supports the provision of sexuality education to in-school and out-of-school youth. The
Programme national multisectoriel de lutte contre la mortalit
maternelle, n
onatale et infanto-juv
nile au Cameroun: plan strat
gique, 2014-2020
addresses the roles that the Ministries of Education and Health have in equipping young people with knowledge on sexual and reproductive health (SRH).
The
Plan strat
gique national de la sant
des adolescents et des jeunes au Cameroun, 2015-2019
aims to strengthen social mobilization in favor of youth SRH and includes an objective to improve adolescent and youth knowledge of issues that impact their reproductive health. Activities include spreading information in formal and informal settings:
OS2 : Am
liorer le niveau de connaissances des A/J [adolescents/jeunes] sur les questions de SRAJ [sant
reproductive des adolescents et des jeunes]
2.1
laborer les outils techniques et didactiques en mati
re de SRA [sant
reproductive des adolescents] avec l
implication active des jeunes
2.2 Produire et diss
miner les outils d
IEC [Information, Education et Communication] /CCC [Communication pour le Changement de Comportement]
2.3 Former les Leaders des jeunes et les responsables des structures d
encadrement des jeunes en techniques de communication en mati
re de SRAJ.
2.4 Mener des activit
information et de sensibilisation des A/J en mati
re de SRAJ.
2.5 Renforcer l
gration de la th
matique SRAJ (EVF [
ducation
la vie de famille]/EVA/EMP/VIH/SIDA) dans les programmes d
ducation des jeunes, en milieu scolaire et extra- scolaire
The
Plan op
rationnel de planification familiale, 2015-2020
has a detailed strategy to increase youth knowledge of reproductive health in formal and informal settings. The strategy includes the use of information and communication technology to raise awareness among young people, the implementation of SRH education in schools, and strengthening education through health clubs in schools, including peer educators, with a focus on adolescent girls and young people :
Strat
gie D3 : Initiation des strat
gies novatrices de communication en direction des adolescents et jeunes scolaris
s et non scolaris
s
Activit
D3.1 : Utilisation des pour sensibiliser les jeunes
Activit
D3.2 : Intensification de l
enseignement de la SSR [sant
sexuelle et reproductive] en milieu scolaire en synergie avec le minist
re en charge de l
Education (MINSEC, MINSUP, MINFOP)
Activit
D3.3 : Sensibilisation des adolescentes et jeunes par l
interm
diaire des pairs
ducateurs et clubs sant
Activit
D3.4 : Sensibilisation des jeunes du secteur informel et du milieu rural sur les questions de SSR
travers les associations des jeunes (socio-
ducatives, culturelles et sportives) en synergie avec le MINJEC
The four activities outlined in the
Plan operationnel
show a commitment to reaching across formal and informal sectors, including sharing information through mobile phone lines, websites, health clubs, and youth associations. The third and fourth activities both integrate a focus on gender and support links to SRH services:
Sensibilisation des adolescentes et jeunes par l
interm
diaire des pairs
ducateurs et clubs sant
Pour le repositionnement de la PF et une implication des adolescentes et jeunes, il sera n
cessaire de renforcer l
ducation par les clubs sant
au niveau des
coles et les pairs
ducateurs de tous les milieux extrascolaires.
...
Il y aura aussi l
identification des jeunes capables de porter les messages de la SR [sant
reproductive] /PF aux autres jeunes. Il sera organis
deux fois par an une grande activit
culturelle et sportive avec des moments de sensibilisation sur la PF et si possible l
offre des services aux adolescentes et jeunes en marge de l
activit
.
Cameroon
s policy environment is supportive of sexuality education but does not reference all nine of the United Nations Population Fund
s (UNFPA
s) essential components of comprehensive sexuality education (CSE). Therefore, Cameroon is placed in the yellow category for this indicator. Going forward, additional sexuality education policies should consider all nine UNFPA essential components of CSE.
The three service-delivery elements of youth-friendly contraceptive services are mentioned in Cameroon
s policy environment.
The
Plan strat
gique national de la sant
des adolescents et des jeunes au Cameroun, 2015-2019" mentions youth
s right to confidentiality and privacy while seeking services:
Respect des droits humains
: Le respect des droits humains sous-tend que, pour toute r
alisation des programmes de d
veloppement, l
tre humain soit plac
au centre des interventions. Sp
cifiquement pour les adolescents et jeunes, il s
agit du droit
information,
la confidentialit
et l
anonymat, la s
curit
des soins, au libre choix,
intimit
, au bien-
tre, la dignit
, etc.
The "Normes et standards en SR-PF au Cameroun, 2018" expand on the right to confidentiality and privacy by including the requirement that providers must guarantee confidentiality while offering FP services:
2.1.5. Droit
la l
intimit
et
la confidentialit
Le droit
l'intimit
et
la confidentialit
stipule que :
- Les locaux doivent garantir l'intimit
et la confidentialit
des prestataires.
- Les prestataires doivent respecter l'intimit
du client(e).
- L'acc
s au fichier m
dical doit
tre strictement r
serv
aux prestataires de services et aux autres personnes autoris
es.
- Le prestataire veille dans la mesure du possible,
ne pas
tre perturb
durant la consultation.
- Tout le personnel doit respecter le secret professionnel.
- Le personnel m
dical doit toujours prendre soin d'expliquer la pr
sence d'une tierce personne durant la consultation et solliciter l'avis du client(e) avant d'autoriser la pr
sence de cette tierce personne.
3.1 Normes pour la planification familiale.
3.1.4. Cibles de la PF
: Il s
agit des femmes en
ge de procr
er, des hommes et des adolescent(e)s et des jeunes.
3.1.5. L
organisation du travail
...
Les prestataires doivent veiller
l'organisation du travail et des locaux afin de garantir la confidentialit
dans l'offre de services de PF. L'organisation des locaux et des services doit permettre de garantir cette confidentialit
ainsi que le respect de la dignit
des clientes depuis la consultation, l'achat des produits, jusqu'
l'administration de la m
thode.
The "Plan strat
gique
also includes specific objectives to build the capacity of providers and other health facility personnel to offer youth-friendly RH services, including the provision of modern contraceptives:
3.5.2. Axe strat
gique II : Renforcement de l
offre de service de SRAJ [sant
reproductive des adolescents et des jeunes
de qualit
.
OS1 : Introduire les services sanitaires appropri
s aux A/J [adolescents/jeunes] dans au moins 25% des formations sanitaires de chaque district de sant
.
OS2 : Renforcer les capacit
s en SRAJ de tous les gestionnaires et les prestataires.
OS3 : Introduire les modules de SRAJ dans les curricula de formation des personnels m
dicaux et param
dicaux.
Finally, the
Plan strat
gique national de
la sant
de reproduction, maternelle n
onatale et infantile, 2014-2020," the "Plan op
rationnel de planification familiale, 2015-2020," and "Health Sector Strategy, 2016-2027" all outline strategies to provide services at free or reduced cost.
The
Plan strategique
includes lifting financial barriers for reproductive health, including free annual appointments in schools:
| 2 : Levee barri
res financi
res |
Gratuit
des visites m
dicales annuelles dans les coll
ges, lyc
es et universit
s |
The
Health Sector Strategy, 2016-2027
aims to ensure services are adapted to young people
s needs and states that providing free or subsidized services will help improve the use of contraceptives:
Implementation Strategy 1.4.3: Improving FP service delivery and use:
Improving the availability of FP services shall be done through:
(i) scaling up integrated FP service delivery;
(ii) improving the availability of inputs through better management of the supply system and the establishment of an FP support fund;
(iii) capacity building of human resources in FP to make up for the significant shortage of trained personnel;
(iv) development of FP services adopted to the youth and adolescents. It is for this purpose that inventories will be made for a good mapping of the needs of quality inputs and human resources.
As concerns improving the use of contraceptives, it will be achieved through: ...
(ii) removal of financial barriers (subventions or even free healthcare
for vulnerable targets) and socio-cultural (religious beliefs, disinformation);
Cameroon has a strong policy environment for the provision of youth-friendly FP services and is placed in the green category for this indicator.
The
Plan strat
gique national de la sant
des adolescents et des jeunes au Cameroun, 2015-2019
includes a strategic goal to strengthen social mobilization around youth reproductive health:
3.5.1. Axe strat
gique I : Renforcement de la mobilisation sociale autour de la SRAJ
[sant
reproductive des adolescents et des jeunes].
OS1 : Am
liorer la communication int
e pour susciter la prise de conscience sur les probl
mes de SRAJ au sein de la communaut
lus, d
cideurs, soci
civile, responsables et Leaders)
OS2 : Renforcer le dialogue parents/enfants sur la SRAJ.
The
Plan strat
gique
stresses the urgent need for social mobilization in favor of youth-friendly services within communities:
La communication portant sur la sant
de reproduction reste insuffisante et prioritairement faite par les prestataires de soins et les enseignants. Or plusieurs autres personnes comme les parents, les leaders communautaires ont
galement la responsabilit
assurer quotidiennement l
ducation de cette cible. D
s lors, il appara
t urgent pour une large mobilisation sociale en faveur de la SAJ
[sant
des adolescents et des jeunes] d
liorer la communication int
e. Celle-ci aura comme principal objectif de susciter une prise de conscience sur les probl
mes de SRAJ au sein des communaut
s. La pertinence d
une telle action repose sur le r
le pr
pond
rant de ces diff
rents acteurs sur l
ducation et le processus de socialisation des A/J [adolescents/jeunes] au niveau familiale voire communautaire.
The
Health Sector Strategy, 2016-2027
aims to improve demand for FP services by strengthening the role that men play in FP promotion:
Implementation Strategy 1.4.2: Improving the demand for FP services
Improving the demand of FP services will be achieved through the development of the following interventions: (i) interpersonal and mass communication in favour of FP to raise awareness on the availability of FP services at the operational level; (ii) strengthening the participation of men as partners in the promotion of FP especially in cultures where women have little decision-making power over their reproductive health.
The
Plan op
rationnel de planification familiale, 2015-2020
includes a detailed strategy to strengthen men as partners in promoting reproductive health. While the strategy does not specifically target youth FP, it includes piloting husbands
schools and promoting family planning among men in agricultural groups:
Strat
gie D2 : Renforcement de l
implication des hommes comme partenaires dans la promotion de la SR
[sant
reproductive] en g
ral et en particulier de la PF
Les hommes sont des d
cideurs cl
s mais ils ont souvent peu d'int
t pour la PF ou qu'ils s'y opposent. Dans certaines localit
s, l
environnement socioculturel influence les comportements qui favorisent les attitudes pro-natalistes. Cependant, certains pays ont men
s, avec succ
s, les hommes
devenir des champions de la PF. La strat
gie de l
Engagement Constructif des Hommes (ECH) sera
labor
e et diss
e. Les organisations paysannes la coordination de Cameroon Development Cooperation (CDC), Farmers groups, PALMOR, SODECOTON, etc... seront impliqu
es dans la sensibilisation des hommes sur la PF. De la m
me mani
re l
approche de l
cole des maris en exp
rimentation sera
tendue dans plusieurs districts.
The "Programme national multisectoriel de lutte contre la mortalit
maternelle, n
onatale et infanto-juv
nile au Cameroun: plan strat
gique, 2014-2020" looks to mainstream gender to strengthen community mobilization and generate demand for the use of health services by women and young people, with an emphasis on the involvement of men, traditional and religious leaders, and young boys. The
Programme national multisectoriel
also aims to take gender into account when implementing its objectives:
Les besoins sp
cifiques des femmes et filles selon leurs statuts devront
tre pris en compte dans la mise en
uvre du PLMI [programme national multisectoriel de lutte contre la mortalit
maternelle, n
onatale et infanto-juv
nile]. Un accent devra
tre mis sur l
implication des hommes, des leaders traditionnels et religieux et des jeunes gar
ons. Cette implication visera les aspects pr
ventifs de lutte contre la mortalit
maternelle et infantile mais
galement l
accompagnement et la prise en charge psycho sociale et la r
insertion socio
conomique des femmes et filles affect
es par les complications li
la mortalit
maternelle.
La prise en compte des sp
cificit
s de genre dans le PLMI concerne par ailleurs la d
finition des activit
s visant la r
duction des discriminations et des violences bas
es sur le genre y compris les pratiques socioculturelles limitant la demande (et l
s) des femmes et des filles aux services et soins de SRMNI. Un accent devra
tre mis sur la jouissance par les femmes et les filles de leurs droits reproductifs, tout en int
grant les besoins des hommes et jeunes en mati
re de PF afin qu
ils soient des parties prenantes actives
la mise en
uvre du PLMI.
While Cameroon
s policies address the need to build community support for youth FP services and to address gender norms, the policies lack a detailed strategy for building an enabling social environment specifically for youth FP services. Therefore, Cameroon is placed in the yellow category for this indicator.
The
Loi n
06.005 du 20 juin 2006 bangayassi relative
la sant
de reproduction
states that individuals are entitled to receive all reproductive health services, including FP, without discrimination and without parental or spousal consent:
Art. 7 : Toute personne a droit
une vie sexuelle satisfaisante, en toute s
curit
. Elle a le droit de procr
er et doit
tre libre de le faire au rythme de son choix.
Le droit de procr
er implique l
information et l
utilisation des m
thodes de planification familiale conform
ment aux normes prescrites ; l
des services de sant
devant permettre aux femmes de mener
bien grossesse et accouchement, et donnant aux couples toutes les chances d
avoir des enfants en bonne sant
.
Art. 14 : Les patients sont en droit de recevoir tous les soins de sant
en mati
re de la reproduction sans discrimination aucun, fond
e sur le sexe, la religion, l
ethnie, l
ge, le statut sanitaire ou tout autre statut. Sauf dispositions l
gales contraires, l
autorisation du partenaire ou de ses parents avant le traitement peut ne pas
tre requise.
The
Politique nationale de la sant
de la reproduction, 2015
continues to support access to contraceptive methods without the need for spousal consent:
2.2.1 La Planification Familiale
Les femmes et les hommes en
ge de procr
er pourront avoir acc
s aux m
thodes contraceptives r
versibles sans recours pr
alable au consentement de leur conjoint. Toutefois, l
accent doit
tre mis sur l
importance du dialogue dans le couple pour l
adoption d
une m
thode contraceptive
;
The reviewed policies support youth access to family planning without spousal and parental consent. The Central African Republic is placed in the green category for this indicator.
CAR lacks any policy addressing non-medical provider authorization for youth FP services and is therefore placed in the gray category for this indicator.
The
Loi n
06.005 du 20 juin 2006 bangayassi relative
la sant
de reproduction
guarantees equitable access to sexual and reproductive health care regardless of age:
Art. 7 : Toute personne a droit
une vie sexuelle satisfaisante, en toute s
curit
. Elle a le droit de procr
er et doit
tre libre de le faire au rythme de son choix. Le droit de procr
er implique l
information et l
utilisation des m
thodes de planification familiale conform
ment aux normes prescrites ; l
des services de sant
devant permettre aux femmes de mener
bien grossesse et accouchement, et donnant aux couples toutes les chances d
avoir des enfants en bonne sant
.
Art. 8 : Tous les individus sont
gaux en droit et en dignit
en mati
re de la reproduction. Ce droit est universel et fondamental. Il est garanti
tout
tre humain, tout au long de sa vie, en toute situation et en tout lieu. Aucun individu ne peut
tre priv
de ce droit dont il b
ficie sans aucune discrimination fond
e sur l
ge, le sexe, la fortune, la religion, l
ethnie, la situation matrimoniale et sans la moindre coercition ou la violence.
The
Politique nationale de la sant
de la reproduction, 2015
also states that all individuals of reproductive age have the right to family planning services. Because the policies reviewed guarantee access to family planning regardless of age, CAR is placed in the green category for this indicator.
The
Loi n
06.005 du 20 juin 2006 bangayassi relative
la sant
de reproduction
guarantees youth access to sexual and reproductive health care, including FP, regardless of marital status:
Art. 7 : Toute personne a droit
une vie sexuelle satisfaisante, en toute s
curit
. Elle a le droit de procr
er et doit
tre libre de le faire au rythme de son choix. Le droit de procr
er implique l
information et l
utilisation des m
thodes de planification familiale conform
ment aux normes prescrites ; l
des services de sant
devant permettre aux femmes de mener
bien grossesse et accouchement, et donnant aux couples toutes les chances d
avoir des enfants en bonne sant
.
Art. 8 : Tous les individus sont
gaux en droit et en dignit
en mati
re de la reproduction. Ce droit est universel et fondamental. Il est garanti
tout
tre humain, tout au long de sa vie, en toute situation et en tout lieu. Aucun individu ne peut
tre priv
de ce droit dont il b
ficie sans aucune discrimination fond
e sur l
ge, le sexe, la fortune, la religion, l
ethnie, la situation matrimoniale et sans la moindre coercition ou la violence.
Because the law guarantees access to family planning regardless of marital status, CAR is placed in the green category for this indicator.
The
Loi n
06.005 du 20 juin 2006 bangayassi relative
la sant
de reproduction
states that any individual or couple has the right to choose the method of family planning that works for them:
Art. 9 : Tout individu ou tout couple a le droit de d
cider librement et avec discernement, de la taille de sa famille dans le respect des lois en vigueur, de l
ordre public et de bonnes m
urs. Pour ce faire, il a le droit de choisir la m
thode de planification familiale qui lui convient.
The
Loi n
06.005
also states that contraception includes all methods recognized as effective and safe, including modern and traditional methods. An individual has the right to choose from the full range of methods:
Art. 23 : La contraception comprend toutes m
thodes approuv
es, reconnues efficaces et sans danger. Ces m
thodes peuvent
tre modernes, traditionnelles ou populaires. Toute la gamme des m
thodes contraceptives l
gales doit
tre propos
e et disponibles.
Art. 24 : Le droit de d
terminer le nombre d
enfants et de fixer l
espacement de leur naissance conf
chaque individu la facult
de choisir parmi toute la gamme de m
thodes contraceptives efficaces et sans danger, celle qui lui convient.
The
Plan national de d
veloppement sanitaire, 2006-2015
aims to provide a minimum package of activities and includes equipping facilities with contraceptive products, although it provides no details on which products:
Services de sant
en faveur des femmes am
lior
s et disposent d
un paquet minimum d
activit
s selon les normes
- Evaluer les besoins en
quipements en mati
re de MSR [maternit
sans risque], Soins Obst
tricaux et N
onataux d
Urgence (SONU), produits contraceptifs
;
- Equiper les structures en mat
riel
: 8 ordinateurs + accessoires ; 100 tables d
accouchement
; 20 motocyclettes
; produits contraceptifs
;
The "Standards des services de sant
adapt
s aux adolescents et aux jeunes en RCA, n.d." outline the minimum package of services for adolescents and youth along the different tiers of the health system. The
Standards des services
note that all health levels should offer a range of contraceptives (pills, injectables, intrauterine devices, implants, and natural methods) when possible or refer youth to other facilities.
CAR
s policies allow youth to access a range of methods but fall short of clearly stating that long-acting and reversible contraceptives are included in method choice. In the absence of a policy statement that requires health providers to offer short-acting and long-acting reversible contraceptive services to youth, CAR is placed in the yellow category for this indicator.
Although the availability of emergency contraception (EC) is not factored into the categorization of this indicator, none of CAR
s policy documents reference youth access to EC.
The
Education sexuelle compl
te des adolescents et des jeunes: manuel de r
rence de la R
publique centrafricaine
usage des formateurs des formateurs, n.d.
provides a general overview of comprehensive sexuality education (CSE) and details the curriculum modules for implementation. The curriculum manual aims to provide young people with essential skills, accurate knowledge of their rights and gender norms, and sexual and reproductive health and rights and is divided into seven main modules: human development; interpersonal relationships; gender; values and attitudes; sexual behaviors; sexual and reproductive health; and rights and needs.
The
Manuel de reference
plainly states that the curriculum content is based in the core values of human rights:
Les directives sur l'
ducation sexuelle s'appuient sur une approche bas
e sur les droits en mati
re de sexualit
, dont les valeurs sont inextricablement li
es aux droits humains universels. Il n'est pas possible de s
parer les consid
rations portant sur les valeurs des discussions relatives
la sexualit
.
The
Manuel de r
rence" acknowledges that a well-implemented CSE program should have many qualities, including scientifically accurate information, employment of participatory teaching methods, and activities that take cultural values into account and promote decision making and critical thinking. The curriculum
s general objectives provide further information on the
Manuel
focus on scientific information and decision-making:
- B
ficier d'informations exactes sur les droits sexuels et reproductifs chez l
enfant , l
adolescent et les jeunes ; d'informations pour dissiper les mythes ; de r
rences
des ressources et
des services ;
- D
velopper des aptitudes
la vie quotidienne notamment dans le domaine de la pens
e critique, de la communication, de l
coute active, de la n
gociation, du d
veloppement autonome, de la prise de d
cision, de l'estime de soi, de la confiance en soi, de la capacit
s'imposer, de la prise de responsabilit
s, de la capacit
poser des questions et
demander de l'aide, de l'empathie ;
- Cultiver des attitudes et des valeurs positives gr
une ouverture d'esprit ; au respect de soi-m
me et des autres ;
une estime/conscience de soi positive ;
une attitude sans jugement ;
un sens des responsabilit
; a une attitude positive vis-
-vis de leur sant
sexuelle et reproductive.
In addition to containing a module dedicated to gender, the
Manuel de r
rence" acknowledges how the CSE curriculum will aim to eliminate negative norms and taboos related to gender and health:
L
ESC vise avant tout
liminer les normes et st
otypes, ainsi que la discrimination et la stigmatisation, tout en embrassant la diversit
et le respect de l
volution des capacit
s des enfants et des jeunes. Cela exige un effort concert
et soutenu pour contrer le silence et le tabou entourant les questions de sexe, de sexualit
, de genre et de sant
, au profit d
une approche outillant les jeunes pour aborder leur sexualit
de fa
on positive.
The curriculum also addresses the of education to sexual and reproductive health services and other initiatives, strengthening youth advocacy and civic engagement, and ensures cultural relevance in tackling gender inequality.
The "Politique nationale de la sant
de la reproduction, 2015" notes the right of young people to sexual education and family life:
Les jeunes ont droit
ducation
la vie sexuelle,
la vie familiale et l'
ducation
la parent
responsable.
The
Politique nationale
and other major policy documents, including the
Plan national de d
veloppement sanitaire, 2006-2015
and the
Cadre strat
gique national de lutte contre le VIH et le sida, 2012-2016,
note the importance of CSE uptake at all education levels.
While CAR
s CSE curriculum adequately addresses seven of the nine United Nations Population Fund
s (UNFPA
s) essential components, it fails to detail how educators will nurture a safe and healthy learning environment and reach both the formal and informal sectors. CAR is therefore placed in the yellow category for this indicator.
The
Loi n
06.005 du 20 juin 2006 bangayassi relative
la sant
de reproduction" guarantees an individual
s right to access reproductive health services at an affordable cost and to privacy of information:
Art. 13 : Tout individu ou tout couple a le droit de b
ficier des soins de sant
de qualit
et de services s
rs, efficaces, accessibles et
un co
t abordable.
Art. 15 : Aucune information concernant la sant
du patient ou de l
usager ne doit
tre divulgu
e sans autorisation expresse de celui-ci. Le patient a le droit de conna
tre les informations dont le prestataire de soins habilit
dispose sur sa personne.
The
Loi n
06.005
also states that government health facilities must be adapted to the needs of specific groups, including young people:
Art. 19 : L
Etat et les collectivit
s examinent et mettent en place les structures int
es des soins de sant
de la reproduction. Celles-ci doivent
tre adapt
es aux besoins sp
cifiques de tous, y compris des jeunes. Ces structures doivent poursuivre un but non lucratif, sous r
serve des dispositions sp
cifiques concernant les structures priv
es de prestation de services.
The
Politique nationale de la sant
de la reproduction, 2015
supports continued provider training in sexual and reproductive health, but it is not specific to youth FP or the prevention of judgment or bias:
2.4.8 Formation
Les prestations de SR [sant
reproductive]
tant soutenues entre autres par des connaissances en pleine
volution, la formation en cours d
emploi et le recyclage des prestataires seront renforc
s. Toute formation continue du personnel socio-sanitaire en SR devra r
pondre
des besoins de formation identifi
s. L
enseignement des composantes de SR sera renforc
dans la formation de base et le recyclage du personnel de sant
et des agents sociaux.
The "Standards des services de sant
adapt
s aux adolescents et aux jeunes en RCA, n.d." outline the standards expected of providers working with adolescents and young people, including the right of adolescents to access quality health services without any discrimination related to their age and a guarantee of privacy and confidentiality:
- Le respect des droits humains et en particulier le droit des adolescents et des jeunes
s aux services de sant
de qualit
sans discrimination aucune li
leur
ge, sexe, religion ou conditions sociales ;
- La prise en compte de la dimension Genre et des valeurs socioculturelles ;
- Le respect des politiques, strat
gies et programmes nationaux existants ;
- Le respect des r
gles d
thique m
dicale ;
- La garantie de la confidentialit
dans le respect de la vie priv
e des adolescents et des jeunes ;
- L
assurance que les interventions reposent sur des bases scientifiques prouv
es ;
- L
appropriation par la communaut
et l
implication de toutes les parties prenantes y compris les adolescents et les jeunes eux-m
mes ;
- L
gration dans les autres secteurs de d
veloppement en privil
giant l
approche multisectorielle.
The "Standards des services" go on to outline the five standards for adolescent and youth health care, including providers having the knowledge and attitudes required to provide services adapted to young people:
Standard II : Tous les prestataires du PPS [point de prestations de services] ont les connaissances, les aptitudes et les attitudes requises, pour offrir des services adapt
s aux besoins des adolescents et des jeunes.
Raisons d
tre :
- Les adolescents et les jeunes peuvent
tre tenus
cart des services de sant
en raison de l
absence d
orientation des prestataires en SAJ
[sant
des adolescents et des jeunes] ;
- Les adolescents et jeunes d
plorent le mauvais accueil et la discrimination dont ils font l
objet lorsqu
ils d
sirent des services de sant
;
- Les services de sant
peuvent
tre de mauvaise qualit
en raison d
un manque de qualification ou de motivation des prestataires y compris le personnel de soutien ;
- Les prestataires sortants des
coles ne re
oivent pas une formation appropri
e en SAJ.
The
Standards des Services
continue to outline the minimum package of services for adolescents and young people
which includes family planning
and the actions to be taken at each level of the health system to reach these standards, including training of providers to have the knowledge, skills, and attitudes required to offer services tailored to youth needs.
While the current policy environment outlines standards for providers to enforce confidentiality and audio/visual privacy and train providers to have the appropriate attitudes for youth seeking FP services, it fails to adequately reference the three contraceptive service-delivery elements. To move to a fully supportive policy environment, future policies should link training providers in youth FP services to prevent bias and clarify that affordable costs include no cost or subsidized FP services. CAR is placed in the yellow category for this indicator.
The
Politique nationale de la sant
de la reproduction, 2015
acknowledges the role community actors can play in promoting reproductive health:
1.5.3 R
le des acteurs externs
Les communaut
s et les collectivit
s seront impliqu
es dans le processus de planification, d
identification des besoins prioritaires, et de toutes les activit
s de promotion de la sant
de la reproduction.
While the most recent reproductive health policy acknowledges gender in its basic principles, including an acknowledgment of the need for a gender approach in implementation, the policy does not identify activities to build support within the community and address gender roles, as the previous version did.
The
Education sexuelle complete des adolescents et des jeunes
: manuel de r
rence de la R
publique centrafricaine
usage des formateurs des formateurs, n.d.
supports sensitizing religious leaders on the importance of family planning for adolescents and youth:
Obstacles
la Contraception
Au niveau Religieux
Strat
gies : Impliquer les chefs religieux dans les activit
s de PF
Les convaincre du bienfond
de l
utilisation des m
thodes contraceptives cliniques
The
Standards des services de sant
adapt
s aux adolescents et aux jeunes en RCA, n.d.
identify community leaders and parents as groups to target to improve youth-friendly health services:
1.1 Objectif g
ral
Am
liorer l
s des adolescents et des jeunes
des services de sant
adapt
leurs besoins ainsi que leur prise en charge en RCA.
2.2 Cibles secondaires
- Les groupes cibles secondaires sont constitu
s de :
- Les parents ;
- Les enseignants ;
- Les prestataires des services de sant
;
- Les jeunes pairs
ducateurs et encadreurs de jeunes ;
- Les leaders communautaire
The
Plan strat
gique national de s
curisation des produits de sant
de la reproduction et de programmation holistique des pr
servatifs en R
publique centrafricaine, 2013-2017
recommends sensitizing community leaders (including religious leaders, traditional healers, and mothers) on the importance of condom use, but it does not detail any activities.
The
Plan national de d
veloppement sanitaire, 2006-2015
outlines a strategic objective to avail quality reproductive health services with male and community support. As part of a minimum package of activities in health facilities, the government of the Central African Republic aims to:
- Sensibiliser les communaut
s sur les bienfaits des services de SR, en Genre
;
- Mobiliser et faire participer les communaut
s aux efforts d
lioration de la qualit
des services de sant
en SR.
While the National Health Plan acknowledges that the current environment in CAR does not adequately address gender issues in health strategies, it does not propose interventions to address gender and social norms. Additional documents acknowledge the roles that community leaders can play and the need to address gender norms but do not connect community engagement to youth contraceptive use and do not detail specific intervention activities. . As no policy exists to build an enabling social environment for youth FP services, CAR is placed in the gray category for this indicator.
Chad
s policy environment does not specifically prohibit parental and spousal consent for youth access to FP services. Until it addresses consent from a third party in a future policy, Chad is placed in the gray category for this indicator.
No law or policy was identified that requires providers to provide medically advised FP services to youth without personal bias or discrimination. Chad is placed in the gray category for this indicator.
The
Loi n
006/PR/2002 du 15 avril 2002 portant promotion de la sant
de reproduction
guarantees the right to reproductive health regardless of age:
Chapitre 2 - Des principes et droits en mati
re de sant
de la reproduction
Art.3.- Tous les individus sont
gaux en droit et dignit
en mati
re de sant
de reproduction sans discrimination aucune fond
e sur l
ge, le sexe, la fortune, la religion, l
ethnie, la situation matrimoniale ou sur toute autre situation...
Art.6.- Tout individu, tout couple a droit
information,
ducation et aux moyens n
cessaires relatifs aux avantages, aux risques et
efficacit
de toutes m
thodes de r
gulation des naissances.
Because these policies address access to FP services regardless of age, Chad is placed in the green category for the indicator.
The
Loi n
006/PR/2002 du 15 avril 2002 portant promotion de la sant
de reproduction,
which identifies FP as part of sexual and reproductive health services, guarantees the right to reproductive health services regardless of marital status:
Chapitre 2 - Des principes et droits en mati
re de sant
de la reproduction
Art.3.- Tous les individus sont
gaux en droit et dignit
en mati
re de sant
de reproduction sans discrimination aucune fond
e sur l
ge, le sexe, la fortune, la religion, l
ethnie, la situation matrimoniale ou sur toute autre situation.
Art.6.- Tout individu, tout couple a droit
information,
ducation et aux moyens n
cessaires relatifs aux avantages, aux risques et
efficacit
de toutes m
thodes de r
gulation des naissances.
Chad is placed in the green category for this indicator as its policies support youth access to FP regardless of marital status.
The
Loi n
006/PR/2002 du 15 avril 2002 portant promotion de la sant
de reproduction
guarantees young people
s access to reproductive health services regardless of age, and further details that these services include all FP methods and family planning services:
Chapitre 4 - Des soins et services de sant
de reproduction
Art.13.- Par soins et services de sant
de la reproduction, on entend notamment :
- L
orientation, l
information, l
ducation, la communication, la recherche, les moyens, les m
thodes et, de mani
re g
rale, tous les services en mati
re de planification familiale
While Chad
s reproductive health law explicitly mentions youth
s right to family planning methods, it is ambiguous in its scope. For Chad to move into the green category, it needs to ensure that long-acting and reversible contraceptives are offered and available among the essential contraceptive options for youth. Chad is placed in the yellow category for this indicator.
Although the availability of emergency contraception (EC) is not factored into the categorization of this indicator, note that no reviewed policies reference youth access to EC.
The
Plan d
actions quinquennal de mise en
uvre de la politique nationale genre, 2019-2023
includes a strategic objective to reach equal and equitable access to basic social services by men and women, including promoting rights in reproductive health through education:
Dans ce cadre, des actions de plaidoyer, de sensibilisation et de renforcement des capacit
s sont
velopper
chelle de l
ensemble des provinces. Par ailleurs il est retenu de promouvoir des initiatives visant
satisfaire les besoins sp
cifiques de filles et des gar
ons, des hommes et des femmes dans le secteur de l
ducation, de la formation et de l
alphab
tisation, ce ci de mani
er des conditions favorables de maintien et de succ
s des filles, au m
me titre que les gar
ons dans le syst
me scolaire formel et les femmes au m
me titre que les hommes dans l
ducation non formelle et l
alphab
tisation. Par ailleurs il s
agira de contribuer
lioration de la Sant
de la Reproduction et
la r
duction de la mortalit
maternelle et n
onatale de mani
assurer aux hommes et aux femmes des services de sant
de la reproduction de qualit
de fa
duire significativement les risques de mortalit
la maternit
et
permettre
chacune et
chacun d
avoir une vie saine et responsable.
While the
Plan d
action
supports sexuality education among young people and acknowledges the benefits of education to young girls, no policies were identified that addressed sexuality education in detail. Chad is placed in the gray category for this indicator but could move into a more supportive environment by mandating sexuality education in a national policy and including each of the nine UNFPA elements of comprehensive sexuality education.
The
Loi n
006/PR/2002 du 15 avril 2002 portant promotion de la sant
de reproduction
guarantees an individual
s right to access affordable reproductive health services:
Art.8.- Tout individu, tout couple a le droit d
der
des services de sant
de proximit
rs, efficaces, abordables et acceptables.
The "Politique nationale de sant
, 2016-2030" looks to improve health care delivery to young people through reproductive health services adapted to their needs:
Intervention 2 : Am
lioration de la prestation des soins de qualit
aux femmes, aux jeunes et aux enfants. Il s
agit de :
- Promouvoir la sant
des jeunes et des adolescents en cr
ant des centres de sant
reproductive r
pondant aux besoins des jeunes et des adolescents.
The
"Plan national de d
veloppement sanitaire, 2018-2023" acknowledges that adolescent health policy is limited in the country. As one of its strategic goals, the
Plan national
aims to promote the health of young people and adolescents through providing health services to youth as part of the package of services at all health levels. To support this goal, the
Plan national
suggests defining policies and strategic plans with interventions, such as youth centers and counseling for youth:
Action 22.1.1 : D
finir les politiques, plans strat
giques, les normes relatives
la sant
des jeunes, des adolescents, des personnes
es et des personnes handicap
es.
La d
finition des politiques et des plans strat
giques de sant
scolaire, de la sant
des adolescents et des personnes
es favorisera leur d
veloppement. Dans la mise en
uvre de ces politiques seront mieux organis
s les services de sant
existants
disposer des centres de conseils et d
coute des jeunes et adolescents et des centres de r
ducation fonctionnelle. A travers cette action, on renforcera le service national d
hygi
ne scolaire et universitaire en cr
ant progressivement des services r
gionaux dans les 23 r
gions pour mettre en
uvre un paquet de services d
fini.
Once adolescent health policies, plans, and standards are in place, the next objective is to strengthen the capacities of health personnel to provide services to young people and adolescents:
Action 22.1.3 : Renforcer les capacit
s du personnel de sant
dans la prise en charge des probl
mes de sant
des adolescents, des jeunes, des personnes
es et des personnes handicap
es.
Une fois les politiques, plans strat
giques et normes relatives
la sant
des adolescents, des jeunes, des personnes
es et des personnes handicap
es,
labor
s et adopt
s, le personnel de sant
sera form
tous les niveaux de la prise en charge et les formations sanitaires
quip
es cons
quemment pour assurer une prise en charge efficace des probl
mes de sant
de ces cat
gories de la population. Ce renforcement des capacit
s devra se traduire entre autres par la prise en compte des interventions relatives
la sant
des adolescents, des jeunes, des personnes
es et des personnes handicap
es, dans les plans op
rationnels annuels.
The
Plan national
acknowledges that the availability of FP services in the country is high, but facilities have low operational capacity. To remedy this problem, the
Plan national
proposes an intervention to train health personnel in counseling to better present methods of contraception and their side effects and ensure that the FP guidance is included in medical training at all levels:
La disponibilit
des services de PF est assez
e, mais leur capacit
rationnelle est faible. Pour pallier
cette situation, le personnel de sant
sera form
en conseil afin de mieux pr
senter les diff
rentes m
thodes de contraception et les effets ind
sirables. Les directives relatives
la PF MSP - Plan National de D
veloppement Sanitaire : PNDS3 2018-2021 - Tchad seront mises
disposition des formations m
dicales de tous les niveaux. L
approvisionnement r
gulier des intrants de la PF sera assur
.
The reviewed policy documents recognize Chad
s nascent status in youth-friendly FP service provision. By guaranteeing the right to affordable FP services and acknowledging the need to train providers to provide services to youth, Chad has a promising but insufficient policy environment. To move to a fully supportive policy environment, policies should link provider training to issues of judgement and ensure confidentiality and audio/visual privacy for youth accessing FP services. Chad is placed in the yellow category for this indicator.
The
Plan d
actions quinquennal de mise en
uvre de la politique nationale genre, 2019-2023
acknowledges the gender inequities that affect women
s control over reproductive health decisions. The policy reinforces the right to health
including reproductive health
as a guiding principle. One of the action plan
s strategic objectives is to reduce gender inequities in access to basic social services and limit traditional practices that hamper young people
s access to sexual and reproductive health care:
Dans ce cadre des actions de plaidoyer, de sensibilisation et de renforcement des capacit
s sont
velopper
chelle de l
ensemble des provinces. Par ailleurs il est retenu de promouvoir des initiatives visant
satisfaire les besoins sp
cifiques de filles et des gar
ons, des hommes et des femmes dans le secteur de l
ducation, de la formation et de l
alphab
tisation, ce ci de mani
er des conditions favorables de maintien et de succ
s des filles, au m
me titre que les gar
ons dans le syst
me scolaire formel et les femmes au m
me titre que les hommes dans l
ducation non formelle et l
alphab
tisation. Par ailleurs il s
agira de contribuer
lioration de la Sant
de la Reproduction et
la r
duction de la mortalit
maternelle et n
onatale de mani
assurer aux hommes et aux femmes des services de sant
de la reproduction de qualit
de fa
duire significativement les risques de mortalit
la maternit
et
permettre
chacune et
chacun d
avoir une vie saine et responsable.
The first action under this objective to reach equal and equitable access to basic social services is to eliminate harmful traditional practices through education of girls and boys:
Act 3.1.1: Rendre sensible au genre le Plan, les Strat
gies et programmes d
ducation formelle et non formelle, de formation professionnelle et d'alphab
tisation int
grent les questions de genre et favorise la r
duction des in
galit
s entre filles et gar
ons
The second action under this objective is to contribute to improving reproductive health and reducing maternal morbidity:
Act 3.2.2: Concevoir et mettre en oeuvre des strat
gies nationales et notamment provinciales de lutte contre la mortalit
maternelle et n
onatale en vue de l'acc
s effective des femmes, des adolescentes et des jeunes
des services de sant
sexuelle et reproductive de qualit
While the
Plan d
actions
acknowledges gender and social norms within reproductive health and proposes actions, it does not specifically target interventions around youth family planning. For Chad to create an environment that is fully supportive of youth FP, new policies should specifically outline a strategy to link service delivery with activities that build support for youth FP in communities and link gender strategies to youth FP. Chad is placed in the gray category for this indicator.
The
Plan d
action national budg
de planification familiale, 2015-2020
explains that provider and parental judgment toward adolescents, particularly unmarried adolescents, is a barrier to accessing FP services:
Quant aux adolescents et jeunes non en union, ils craignent de rencontrer leurs parents et d
autres adultes dans les points d
la PF et jugent que leur utilisation de la PF est mal per
ue par les prestataires qui pr
rent offrir les m
thodes uniquement aux femmes en union.
C
te d
Ivoire
s policy environment, however, does not adequately prohibit parental and spousal consent. C
te d
Ivoire should consider addressing these forms of external authorization unequivocally in future legislation but is now placed in the gray category for this indicator.
The
Standards des services de sant
adapt
s aux adolescents et aux jeunes en C
te d
Ivoire, n.d.,
which include contraception in the minimum package of services, emphasize the importance of providers having adequate skills and attitudes for youth-friendly service provision:
Standard II : Tous les prestataires du PPS [points de prestations de service] ont les connaissances, les aptitudes et les attitudes requises pour offrir des services adapt
s aux besoins des A&J [adolescent et jeune].
Raisons - d
tre :
- Les A&J d
plorent le mauvais accueil, la stigmatisation et la discrimination dont ils font l
objet lorsqu
ils d
sirent les services de sant
de la reproduction ;
- Les prestataires des PPS n
ont pas souvent la formation requise pour offrir des services adapt
s aux besoins des A&J au cours de leur formation de base.
Because the
Standards des services
say definitively that providers must have an attitude void of stigma and discrimination, C
te d
Ivoire is placed in the green category for this indicator.
The
Document de politique nationale de la sant
de la reproduction et de planification familiale (2
dition), 2008
guarantees equitable access to sexual and reproductive health (SRH) care regardless of age:
Au regard de ces droits, la politique nationale de la SSR [sant
sexuelle et reproductive] exige l
quitable
information et aux soins sans distinction de sexe, d
ge, de race, d
ethnie, de religion, de r
gion, de classe sociale. Elle insiste
galement sur le droit pour tout individu de d
cider librement, de fa
clair
e, de sa sexualit
et de sa reproduction.
Dans cette optique, la pr
sente d
claration de politique nationale de la sant
de la reproduction repose sur des valeurs essentielles suivantes : la solidarit
quit
thique et le respect de la sp
cificit
du genre.
The
Politique nationale de population, 2015
includes a specific objective to empower women, which will be achieved through promoting universal access to SRH care for women, girls, and young people:
Objectif g
ral 4
Assurer l
autonomisation de la femme et l
quit
de genre
Objectif sp
cifique 4.1
R
duire les in
galit
s de genre et les violences bas
es sur le genre
Pour ce faire, il faut : d
fendre l
s universel
la sant
sexuelle et reproductive, en particulier pour les femmes, les filles et les jeunes, y compris pendant les p
riodes de conflits et de situations d
urgence.
Because these policies address access to family planning services regardless of age, C
te d
Ivoire is placed in the green category for this indicator.
The
Plan d
action national budg
de planification familiale, 2015-2020
explains that provider and parental judgment toward adolescents, particularly unmarried adolescents, is a barrier to accessing FP services:
Quant aux adolescents et jeunes non en union, ils craignent de rencontrer leurs parents et d
autres adultes dans les points d
la PF et jugent que leur utilisation de la PF est mal per
ue par les prestataires qui pr
rent offrir les m
thodes uniquement aux femmes en union.
The
Programme d'orientation sur la sant
des adolescents destin
aux prestataires de soins de sant
, 2006,
a World Health Organization training document officially adopted by the National Program for School and University Health in the Ministry of Health and Public Hygiene for training providers in youth-friendly services, includes guidance on providing contraceptive services to unmarried youth:
Adolescentes non mari
es
...
Les adolescentes, surtout celles qui ont une relation exclusive, peuvent
galement souhaiter utiliser d
autres m
thodes plus durables [que les pr
servatifs]. Les prestataires de services de contraception doivent soutenir cette d
cision.
Because a policy exists that supports youth access to FP for unmarried adolescents, C
te d
Ivoire is placed in the green category for this indicator.
The
Plan strat
gique national de la sant
des adolescents et des jeunes, 2016-2020
describes the minimum package of services for adolescents, which includes contraception but does not specify which methods should be made available.
The
Programme d'orientation sur la sant
des adolescents destin
aux prestataires de soins de sant
, 2006
includes eligibility criteria for all contraceptive methods. However, this document represents outdated World Health Organization (WHO) medical eligibility criteria for intrauterine devices (IUDs) and implants. It includes restrictions for IUDs based on age and parity:
M
thode d
conseill
e aux moins de 20 ans en raison d
un grand risque d
expulsion chez les plus jeunes femmes nullipares
It also includes restrictions for progestin-only injectables based on age:
M
thode d
conseill
e aux moins de 18 ans en raison d
un trouble possible du d
veloppement osseux
For C
te d
Ivoire to move into the green category, it must adopt the updated WHO medical eligibility criteria (2015), which state that these methods are generally safe for youth and nulliparous women and that the benefits of using the methods outweigh any potential risks. As it is currently written, the
Programme d'orientation
discourages providers from providing these methods to youth who fall within the above-mentioned restrictions, rather than clarifying that they are generally safe for young women regardless of age and parity.
Although the availability of emergency contraception (EC) is not factored into the categorization of this indicator, note that the Programme d'orientation also includes EC in the list of methods.
The
Programme national de l
education sexuelle compl
te de C
te d
Ivoire, 2016-2020
describes the country
s comprehensive sexuality education (CSE) program, which includes all nine of the essential United Nations Population Fund (UNFPA) components of CSE.
For example, the CSE program includes an integrated focus on gender through which youth learn about the role of gender norms in society and the impact of gender norms on sexual and reproductive health (SRH):
1. Genre
Promouvoir l
galit
de genre est un imp
ratif moral. Cette unit
aborde efficacement la question du genre, pour les filles comme pour les gar
ons. Elle d
crit le jeu des normes de genre dans la soci
(dans les relations familiales,
cole, dans l
rience de la violence, dans les m
dias et ailleurs) et explique l
effet des r
les de genre sur la sexualit
et la sant
sexuelle.
The CSE program also includes components on improving communication skills and decision-making in SRH:
2. Relations interpersonnelles et communication
Cette composante explique les relations et les liens avec les membres de la famille, les amis, les voisins, les connaissances, le ou la petit(e) ami(e), ses enseignants, ses camarades, etc. Le but de cette composante est d
aider les adolescent(e)s
mieux comprendre leurs relations et
les aborder avec plus de confiance.
3. Valeurs et attitudes
Les jeunes aiment apprendre comment parler de sujets intimes sans g
ne et avec confiance. Il s
agit dans cette unit
de mettre l
accent sur les attitudes et les valeurs telles que le Respect de soi et d
autrui, l
Estime de soi, la prise de d
cisions qui permettent aux adolescents et aux jeunes d
tre confiant en leurs capacit
s afin de b
ficier d
une meilleure sant
et pr
parer un avenir radieux.
The CSE program aims to reach youth in and out of school with information that is culturally and age appropriate:
Fournir des conseils aux acteurs concern
s sur la mani
re d
laborer des mat
riels et des programmes d
ducation sexuelle con
us pour r
pondre aux besoins, culturellement pertinents et adapt
ge des b
ficiaires.
Renforcer les capacit
s des acteurs de l
ducation formelle et non formelle
Cette strat
gie n
cessite l
organisation d
ateliers de renforcement des capacit
s de la communaut
ducative et des partenaires sociaux.
The
Plan acc
de r
duction des grossesses
l'ecole, 2013-2015 - campagne z
ro grossesse
l'
cole en C
te d
Ivoire
which lays the groundwork for the
Programme national,
provides a clear link between sexuality education and gender norms by focusing on empowering girls to stay in school and manage their SRH needs. It also has a strong emphasis on linking sexuality education with youth-friendly services.
In addition to these programs, C
te d
Ivoire plans to publish extensive teaching aids and materials on SRH topics such as early pregnancy and parent-child communication on SRH; contraception and youth rights in SRH; gender-based violence and early marriages; and sexually transmitted infections and HIV/AIDS. The materials will be published for four groups: teacher trainees and primary-school, secondary-school, and college students.
C
te d
Ivoire has a strong policy environment for CSE, including reference to all nine of the United Nations Population Fund
s (UNFPA
s) essential components of CSE, and is placed in the green category for this indicator.
The
Politique nationale de population, 2015
includes a strategy to develop and expand youth-friendly sexual and reproductive health (SRH) services, and the
Plan strat
gique de la planification familiale, 2012-2016
includes an activity to develop standards for youth SRH services.
The
Plan strat
gique national de la sant
des adolescents et des jeunes, 2016-2020
discusses training providers in youth-friendly services, including SRH services. The
Plan strat
gique de la planification familiale
includes specific activities to establish youth-friendly FP services, including training providers. The
Plan d
action national budg
de planification familiale, 2015-2020
acknowledges that adolescents and young people face provider judgment and includes specific activities to develop training manuals, train and supervise providers, and evaluate the performance of centers offering youth-friendly services:
3.1- D
fis en mati
re de demande des services de PF
Quant aux adolescents et jeunes non en union, ils craignent de rencontrer leurs parents et d
autres adultes dans les points d
la PF et jugent que leur utilisation de la PF est mal per
ue par les prestataires qui pr
rent offrir les m
thodes uniquement aux femmes en union. Ils ont un faible leadership et sont faiblement impliqu
s dans les d
cisions qui concernent leur avenir...
Activit
O3.1: Formation des prestataires de 25% des FS [formation sanitaire] pour offrir des services de PF adapt
s aux adolescents et jeunes
- Elaboration/Adaptation des manuels de formation en prise en charge des jeunes et adolescents dans les FS offrant la PF;
- Recensement chaque ann
e de 250 FS appropri
es pour la prise en charge des adolescents et jeunes;
- Organisation annuelle de 10 sessions de formation de 5 jours de 25 prestataires en prise en charge des jeunes au niveau des chefs-lieux de r
gions;
- Suivi des activit
s de formation dans les r
gions;
- Renforcement de l
quipement des FS pour attirer plus d
adolescents et jeunes;
- Am
nagement des services (espace horaire, activit
s, etc.
) pour prendre en compte les besoins des jeunes;
- Supervision des prestations offertes par les prestataires form
s;
- Evaluation de la performance des centres offrant des services aux jeunes.
The
Standards des services de sant
adapt
s aux adolescents et aux jeunes en C
te d
Ivoire, n.d.
include activities to train providers to have an attitude free of stigma and discrimination when providing youth friendly services:
Standard II : Tous les prestataires du PPS [points de prestations de service] ont les connaissances, les aptitudes et les attitudes requises pour offrir des services adapt
s aux besoins des A&J [adolescent et jeune].
Raisons - d
tre :
- Les A&J d
plorent le mauvais accueil, la stigmatisation et la discrimination dont ils font l
objet lorsqu
ils d
sirent les services de sant
de la reproduction ;
- Les prestataires des PPS n
ont pas souvent la formation requise pour offrir des services adapt
s aux besoins des A&J au cours de leur formation de base.
The
Standards des services
also describe the right of youth to privacy and confidentiality when accessing services. The
Plan strat
gique de la planification familiale
and the
Plan strat
gique de la sant
de la reproduction, 2010-2014
include the same activity to advocate for reduced costs for youth SRH services:
Organiser des activit
s de plaidoyer en direction du gouvernement pour la r
duction des co
ts des soins de sant
sexuelle et reproductive de tous les adolescents et jeunes dans tous les
tablissements sanitaires.
C
te d
Ivoire
s policy environment is strong in that it addresses all three elements for youth-friendly services. C
te d
Ivoire is placed in the green category for this indicator.
The
Plan strat
gique de la sant
de la reproduction, 2010-2014
offers a strategy to strengthen the capacity of communities to address youth sexual and reproductive health issues:
Strat
gie 3 : Renforcement des capacit
s des individus, des m
nages et des communaut
s en mati
re de SR [sant
reproductive] des adolescents et des jeunes
Interventions prioritaires
1. D
velopper et mettre en
uvre un plan de communication sur la sant
sexuelle et reproductive des adolescents et jeunes.
2. Renforcer la capacit
des relais communautaires sur la sant
sexuelle et reproductive des adolescents et jeunes.
The
Strat
gie nationale de d
veloppement bas
e sur la r
alisation de l'OMD version 4, 2007-2015
describes plans for community awareness campaigns that focus on reducing pregnancies among girls in school and contain information on contraceptive methods:
En outre, des campagnes de sensibilisation m
dia et communautaires sur la sant
sexuelle et de la reproduction seront men
es pour r
duire les taux d
abandons des filles li
s aux grossesses et accouchements pr
coces. Ces campagnes devront mettre en relief les inconv
nients de la pr
cocit
de la vie sexuelle et des comportements sexuels
risque, les m
thodes contraceptives, etc.
The
Plan national de d
veloppement, 2016-2020
notes that improved FP use depends on empowering women and ensuring schooling for girls:
Les effets escompt
terme
travers la r
alisation de la
volution contraceptive
, ne seront perceptibles que si des progr
s notables sont r
alis
s dans la scolarisation et en particulier la scolarisation des jeunes filles et l
autonomisation de la femme. Ainsi, il sera question
ce niveau, de garantir un meilleur acc
ducation pour toutes les jeunes filles et de favoriser l
autonomisation de la femme
travers des activit
ratrices de revenu.
The
Politique nationale de population, 2015
includes a specific objective to promote universal access to sexual and reproductive health for women and girls:
Objectif g
ral 4 Assurer l
autonomisation de la femme et l
quit
de genre
Objectif sp
cifique 4.1 R
duire les in
galit
s de genre et les violences bas
es sur le genre
Pour ce faire, il faut :
d
fendre l
s universel
la sant
sexuelle et reproductive, en particulier pour les femmes, les filles et les jeunes, y compris pendant les p
riodes de conflits et de situations d
urgence ;
The "Protocole des services de la sant
de la reproduction, n.d." also discusses involving parents, communities, and educators in awareness-raising activities on the sexual and reproductive health of adolescents and young people.
Because C
te d
Ivoire
s policies provide specific intervention activities for building community support for youth FP services and address gender norms, the country is placed in the green category for this indicator.
The
Codes larcier
de la R
publique d
mocratique du Congo, tome I droit civil et judiciaire, 2003
give husbands full control over the legal rights of married women:
Art. 444.
Le mari est le chef du m
nage. Il doit protection
sa femme ; la femme doit ob
issance
son mari.
Art. 448.
La femme doit obtenir l
autorisation de son mari pour tous les actes juridiques dans lesquels elle s
oblige
une prestation qu
elle doit effectuer en personne.
Art. 450.
Sauf les exceptions ci-apr
s et celles pr
vues par le r
gime matrimonial, la femme ne peut ester en justice en mati
re civile, acqu
rir, ali
ner ou s
obliger sans l
autorisation de son mari. Si le mari refuse d
autoriser sa femme, le tribunal de paix peut donner l
autorisation. L
autorisation du mari peut
tre g
rale, mais il conserve toujours le droit de la r
voquer.
In 2018, the Protocol to the African Charter on Human and Peoples
Rights on the Rights of Women in Africa, originally adopted by the African Union in 2003 and also known as the Maputo Protocol, was published in the Journal Officiel de la R
publique D
mocratique du Congo as "Loi n
06/015 du 12 juin 2006 autorisant l
sion de la R
publique d
mocratique du Congo au Protocole
la Charte Africaine des droits de l
homme et des peuples, relatif aux droits de la femme en Afrique.
The
Loi n
06/015
gives women the right to exercise control over their fertility, including the number of children they have and the spacing of births.
Article 14 : Droit
la sant
et au contr
le des fonctions de reproduction.
1. Les
tats assurent le respect et la promotion des droits de la femme
la sant
, y compris la sant
sexuelle et reproductive. Ces droits comprennent :
a) le droit d
exercer un contr
le sur leur f
condit
;
b) le droit de d
cider de leur maternit
, du nombre d
enfants et de l
espacement des naissances;
c) le libre choix des m
thodes de contraception ;
d) le droit de se prot
ger et d
tre prot
es contre les infections sexuellement transmissibles, y compris le VIH/SIDA ;
e) le droit d
tre inform
es de leur
tat de sant
et de l
tat de sant
de leur partenaire, en particulier en cas d
infections sexuellement transmissibles, y compris le VIH/SIDA, conform
ment aux normes et aux pratiques internationalement reconnues ;
f) le droit
ducation sur la planification familiale.
DRC
s public health law, the "Loi n
18/035 du 13 d
cembre 2018 fixant les principes fondamentaux relatifs
organisation de la sant
publique,
legally protects a woman
s ability to choose to use family planning even if her spouse objects.
Article 82
:
Pour les personnes l
galement mari
es, le consentement des deux conjoints sur la m
thode contraceptive est requis.
En cas de d
saccord entre les conjoints sur la m
thode contraceptive
utiliser, la volont
du conjoint concern
prime.
Article 84
:
Les conjoints ont le droit de discuter librement et avec discernement du nombre de leurs enfants, de l
espacement de leurs naissances et de disposer des informations n
cessaires pour ce fair. En cas de d
saccord, la volont
de la femme prime.
While spousal consent is required for contraceptive use, the will of the individual seeking contraception is considered supreme in the case of a disagreement. Similarly, the law encourages spousal discussions on the number of children and spacing of births but, in the case of a disagreement, the woman
s will is supreme.
The
Politique nationale sant
de l
adolescent, 2013
states that the provision of contraceptives to youth is subject to parental consent, which providers must respect. At the same time, somewhat contradictorily, the
Politique nationale
encourages providers to support the self-determination of youth to use reproductive health services. This language does not define the circumstances when parental consent is warranted:
2. La prestation des m
thodes contraceptives chez les jeunes doit
tre subordonn
e le cas
ant par le consentement des parents et l
agent de sant
est tenu
se plier
cette obligation dans le respect des principes d
administration et d
thique de ces m
thodes. Par contre, il faut recommander l
achat des pr
servatifs
la pharmacie et les milieux appropri
s et les pilules dans un centre de sant
.
3. Les prestataires doivent soutenir l
auto-d
termination et le libre choix des adolescents
utiliser les services de sant
de la reproduction dans le respect de leur dignit
et de leur diversit
opinion ou de culture.
More recently, however, the
Democratic Republic of the Congo Family Planning National Multisectoral Strategic Plan, 2014-2020
includes an activity to:
Create a law favorable to family planning, to protect minors and adolescents, and to promote gender.
Recent legal changes, most notably the 2018 public health law, are very promising and have removed the requirement for spousal consent as a barrier. However, because parental consent for youth
s use of contraception is still permitted under the
Politique nationale
, DRC is placed in the yellow category for this indicator. The country has the potential to move into the green category if future laws are enacted that explicitly prohibit parental consent in all cases.
The
Normes de la zone de sant
relatives aux interventions int
es de sant
de la m
re, du nouveau-n
et de l
enfant en R
publique d
mocratique du Congo
: Interventions de sant
adapt
es aux adolescents et jeunes, 2012
detail how providers in health centers should interact with youth when discussing sexual and reproductive health. Providers should ensure confidentiality; use friendly, clear, and respectful communication; avoid judgment; recognize stigma experienced by sexually active youth; and ensure youths
autonomy in decision-making:
3
server un accueil chaleureux et une communication sympathique
adolescent et au jeune.
- Am
nager des espaces / environnement s
r et favorable
entretien.
- Pr
server la confidentialit
et l
intimit
des adolescents et jeunes.
- Adopter des attitudes attrayantes :
- Se montrer ouvert et accessible ;
- Adopter un ton doux et rassurant ;
- Faire attention
votre attitude (geste, mimique, r
action d
tonnement, de r
probation, de condamnation).
- Traiter les adolescents et jeunes avec courtoisie (saluer avec respect et sympathie, offrir le si
ge, se pr
senter).
- User de patience (un certain temps peut
tre n
cessaire pour que les adolescents et jeunes qui ont des besoins particuliers fassent part de leurs probl
mes ou prennent une d
cision).
- Laisser parler l
adolescent ou le jeune sans l
interrompre.
- Eviter de porter de jugement.
- Faire preuve de compr
hension quant aux difficult
s que les adolescents et jeunes
prouvent
parler de sujets touchant
la sexualit
(peur que les parents le d
couvrent, r
probation des adultes et de la soci
).
While this policy explicitly states that providers must be nonjudgmental, open, and respectful, it is within the context of youth-friendly services and does not clearly address provider authorization in youth family planning. DRC is placed in the gray category for this indicator.
The
Loi n
18/035 du 13 d
cembre 2018 fixant les principes fondamentaux relatifs
organisation de la sant
publique
states that any person of reproductive age can access contraceptives.
Article 81
:
Toute personne en
ge de procr
er peut b
ficier apr
s avoir
clair
, d'une m
thode de contraception r
versible ou irr
versible sur consentement libre. En cas de contraception irr
versible, le consentement est
crit, apr
s avis de trois m
decins, et du psychiatre.
Because the public health law addresses access to contraception regardless of age, DRC is placed in the green category for this indicator.
While the
Loi n
18/035 du 13 d
cembre 2018 fixant les principes fondamentaux relatifs
organisation de la sant
publique
recognizes that people of any reproductive age can access contraceptives, it does not explicitly recognize marital status as a criterion for provision or refusal of FP services. Providers and clients may differently interpret this aspect of the law, potentially creating a barrier for youth who want to access contraception. To strengthen the eligibility criteria, the guideline
s eligibility statement should specifically recognize segmented parts of the population, such as married and unmarried youth. Because no policy exists addressing marital status in access to FP services, DRC is placed in the gray category for this indicator.
While the
Politique nationale sant
de l
adolescent, 2013
states that contraceptive methods beyond the preferred method of abstinence must be made available to youth, it only references pills and condoms. The related document,
Paquet d
activit
s PNSA dans la zone de sant
describes plans for FP activities that include youth-friendly contraceptive methods, rather than explicitly including a full range of methods.
The
Standards des services de sant
adapt
s aux adolescents et jeunes, 2014
describe the minimum package of youth-friendly services available at each level of the health system, including the community level. The policy emphasizes providing youth with information on reproductive health, rather than providing them with contraception. One exception is the distribution of oral contraception and condoms to youth, which is included in the minimum package of services at the community level.
The
Plan national de d
veloppement sanitaire recardr
pour la p
riode 2019-2022
: vers la couverture sanitaire universelle" defines the complete list of interventions included in the service package for mothers, children, and adolescents. The list of family planning commodities is exhaustive, ranging from short-term methods to permanent methods, but it identifies the target audience as women of reproductive age who are in union and provides no further language around eligibility.
The
Interventions de sant
adapt
es aux adolescents et jeunes 2012
encourage condom and contraceptive distribution at the community level and indicate in general terms that youth should be informed about how to prevent unwanted pregnancy in visits to health centers. This policy does not describe providing youth with a full range of contraceptive methods.
Unlike some DRC policies, the
Loi n
18/035 du 13 d
cembre 2018 fixant les principes fondamentaux relatifs
organisation de la sant
publique
specifically states that anyone of reproductive age can benefit from both reversible and irreversible contraceptives. Furthermore, the
Loi n
06/015 du 12 juin 2006 autorisant l
sion de la R
publique d
mocratique du Congo au Protocole
la Charte Africaine des droits de l
homme et des peuples, relatif aux droits de la femme en Afrique" binds DRC to the Maputo Protocol, acknowledges a woman
s right to choose any method of contraception.
However, neither policy explicitly mentions youth
s legal right to access a full range of contraception, including long-acting and reversible contraceptives. As DRC does not have a policy extending access to a full range of methods for youth, it is placed in the gray category for this indicator.
Although the availability of emergency contraception (EC) is not factored into the categorization of this indicator, no polices reviewed specifically address youth access to EC.
The
Politique nationale sant
de l
adolescent, 2013
acknowledges the importance of sexuality education and places emphasis on involving youth, parents, schools, and communities. It does not describe any details or components of what a comprehensive sexuality education (CSE) program should include.
The
Democratic Republic of the Congo Family Planning National Multisectoral Strategic Plan, 2014-2020
identifies poor integration of CSE in primary and secondary schools as a key FP demand-generation problem. To address this concern, the strategic plan includes CSE activities to increase demand for FP services among youth:
Integrate Family Planning in the curriculum of secondary schools, higher education and universities and train teachers in comprehensive sexual education for youth and adolescents.
The
Plan strat
gique national de la sant
et du bien-
tre des adolescents et des jeunes, 2016-2020
incorporates a priority focus on activities that support behavior change through CSE in and out of schools:
Les interventions de sant
en faveur des adolescents et des jeunes reposent sur la communication pour le changement de comportement soutenue par l
offre des services de pr
vention. Il s
agit de : l
ducation compl
te sur la sant
reproductive et sexuelle en milieu scolaire et parascolaire.
The "Plan strat
gique" also includes several activities that contribute to CSE, including promoting the core universal value of human rights for adolescents and young people and the provision of safe and healthy learning environments:
Les objectifs sp
cifiques assign
ce Plan sont les suivants :
Am
liorer le niveau de connaissance et les comp
tences des adolescents et jeunes
sur leurs probl
mes sp
cifiques de sant
y compris leurs droits.
D
ici 2020 au moins 50% des adolescents et jeunes adoptent des attitudes et comp
tences favorables au respect de leurs droits dans les 258 zones.
D
ici 2020, 890 espaces d'information et communication pour jeunes sont cr
s dans les 178 zones suppl
mentaires.
Au moins 50% d
adolescents et jeunes participent aux activit
atives et
socio-
ducatives dans les 258 zones d
ici 2020.
The reference to CSE in these strategic plans indicates that the policy environment is promising toward its implementation. However, additional guidelines, in line with the nine United Nations Population Fund (UNFPA) essential components, are necessary to inform the delivery of CSE. The DRC is placed in the yellow category for this indicator.
The policy environment in DRC recognizes the need for youth-friendly FP service provision. The
Democratic Republic of the Congo Family Planning National Multisectoral Strategic Plan, 2014-2020
includes the following activity:
Extend integrated youth-friendly services to all health zones.
Further, the
Plan strat
gique national de la sant
et du bien-etre des adolescents et des jeunes, 2016-2020
references the provision of youth-friendly services and presents plans for how the country aims to adapt the health system to better meet the needs of adolescent and youth. For example, the "Plan strat
gique
explicitly states the importance of having trained staff capable of offering youth services, setting up spaces suitable for young people, and providing contraceptives (defined only as male and female condoms) to this age group.
Ce syst
me devra particuli
rement disposer d
un personnel comp
tent et apte
offrir les soins de sant
cifiques
ce groupe, supprimer le plus possible les barri
res
cette cible sans ressources cons
quentes, am
nager au sein des
tablissements de soins les espaces d'information et communication pour jeunes, fournir r
guli
rement les m
dicaments y compris les contraceptifs et autres intrants (pr
servatifs f
minins et masculins, etc.).
The
Standards des services de sant
adapt
s aux adolescents et jeunes, 2014
recognize the rights of adolescents to quality and confidential health services. These services include distribution of oral contraception and condoms. The
Standards des services
include plans for training providers in youth-friendly services, including having the right attitude, and measuring youth satisfaction with these services:
Standard 3 : Tout prestataire de service a les connaissances, les attitudes et les comp
tences requises lui permettant d
offrir aux adolescents et aux jeunes des services et soins de sant
de mani
re efficace, efficiente et conviviale.
The
Politique nationale sant
de l
adolescent, 2013
describes training providers and ensuring confidentiality in the broader context of adolescent health. However, the policy does not mention plans to offer free or subsidized contraceptive provision to young people. The
Plan strat
gique
encourages use of a discount for
care of adolescents and young people,
but makes no explicit provision for offering contraceptive products or services at no cost or at subsidized costs.
Therefore, the policy environment is understood to be promising but incomplete, and DRC is placed in the yellow category for FP service provision. When expanding youth-friendly service protocols, policymakers should consider including all three service-delivery elements to improve adolescent and youth uptake of contraception.
DRC
s policy environment recognizes building community support for FP. The
Democratic Republic of the Congo Family Planning National Multisectoral Strategic Plan, 2014-2020
includes an activity to mobilize the community surrounding FP. However, the activity is not specific to youth FP.
The
Paquet d
Activit
s PNSA dans la zone de sant
that accompanies the
Politique nationale sant
de l
adolescent, 2013
broadly outlines activities for building community support for youth health in general, such as advocacy aimed at community leaders and community-outreach activities using multimedia/mass media platforms. However, these activities are not specific to building support for youth access to contraception.
The
Plan strat
gique national de la sant
et du bien-etre des adolescents et des jeunes, 2016-2020
has as one of its chief priorities the need to promote the health of young people through empowering communities to find solutions to problems affecting adolescent health:
La promotion de la sant
des jeunes doit viser notamment la responsabilisation des communaut
s de base dans la recherche des solutions sur les probl
mes affectant la sant
des adolescents.
While there is no explicit reference to community support for youth FP services, there is a strategic focus on community mobilization for the promotion of adolescent and youth health, including HIV services, comprehensive sexual and reproductive health education, promotion and availability of condoms, and strengthening the provision of services at the community level:
Axe strat
gique 1 : Communication strat
gique et mobilisation communautaire pour la promotion de la sant
des adolescents et des jeunes
Les interventions de sant
en faveur des adolescents et des jeunes reposent
Il s
agit de : (i) services de conseil et d
pistage volontaire sur le VIH, (ii) l
ducation compl
te sur la sant
reproductive et sexuelle, (iii) la promotion et la disponibilit
des pr
servatifs, (iv) la promotion de la prophylaxie post exposition (en cas de viols), (v) la pr
vention des violences, ainsi que (vi) le renforcement du syst
me communautaire en synergies avec les secteurs nationaux cl
s et de la soci
civile
fournir des services.
The policy environment aims to build community support for youth sexual and reproductive health education and access to condoms but does not reference building community support for youth access to FP services that include a broader range of contraceptive methods. The
Politique nationale
mentions gender, primarily related to gender-based violence, in the context of adolescent health broadly. Because DRC does not include specific interventions related to building an enabling social environment, the country is placed in the yellow category for this indicator.
The
National Adolescent and Youth Health Strategy, 2016-2020
refers to a prohibition against third-party consent requirements for youth seeking contraception:
A law permits adolescents and youth to use contraceptives without third party consent.
However, this law is not identified by name and could not be located. The
National Guideline for Family Planning Services in Ethiopia, 2020
notes that adolescents should receive services without needing to obtain parental consent:
it should be clear that adolescents get service without mandatory parental and guardian authorization/notification. Similarly,
for a woman to get FP services no third-party authorization is required including spousal approval
and providers should affirm that individual decision respected.
Ethiopia
s policies support access to family planning services without parental consent and spousal consent and the country is therefore placed in the green category for this indicator.
Ethiopian policy documents acknowledge the rights of youth to receive family planning services, and the
barrier that provider bias can pose. The
National Adolescent and Youth Health Strategy, 2016-2020
states:
When adolescents and youth attempt to utilize services, they encounter unfriendly environments including breaches in confidentiality, judgmental and disapproving attitudes relating to sexual activity and substance use, and discrimination. This results in failure to provide important services and increase[s] the vulnerability of particular groups.
The policy also outlines multiple priority actions to promote supportive attitudes by providers:
- Build the capacity of health providers to manage and provide AYFHS [adolescent and youth-friendly health services] with a compassionate, respectful and caring manner
- Promote supportive attitudes and behavior by health workers to better engage adolescents and youth in health care services and programs
While these statements are a positive step, the Strategy does not explicitly instruct providers to offer youth-friendly services without judgment or bias. However, the
Standards on Youth Friendly Reproductive Health Services & Minimum Service Delivery Package on YFRH Services: Service Delivery Guideline, n.d.,
which includes FP as part of the youth-friendly service package, mandates that services be provided in adherence with the World Health Organization definitions of adolescent-friendly health services, including:
Adolescent friendly health care providers who
are non-judgmental and considerate[,] easy to relate to and trust worthy.
The
National Guideline for Family Planning Services in Ethiopia, 2020
similarly acknowledges that health professionals must provide unbiased services:
Clients also have the right to access the broadest range of contraceptives to choose and change when they need or encounter any side effects from an earlier method. Health professionals should provide an unbiased counseling service to ensure full, free and informed choice to ensure method mix.
In this context, it should be clear that adolescents get service without mandatory parental and guardian authorization/notification. Similarly,
for a woman to get FP services no third-party authorization is required including spousal approval
and providers should affirm that individual decision respected.
Ethiopia is placed in the green category for this indicator because the policy environment includes provisions discouraging provider judgement or discrimination.
Policies reviewed thoroughly address youth
s right to access FP services, regardless of age.
The
National Guideline for Family Planning Services in Ethiopia, 2020
recognizes a rights-based approach that allows clients to choose the method that is most convenient to them, regardless of age, going as far to direct providers that
if a client is [an] adolescent, use the counseling card to inform [them] that [they] can get any method.
The guideline also underscores
the right to access FP services without discrimination based on age or other nonmedical criteria:
Equity and non-discrimination: Individuals have the ability to access comprehensive contraceptive services free from discrimination, coercion and violence. FP services should not vary by non-medically indicated characteristics, such as age, geography, language, ethnicity, disability, HIV status, income, and marital or other status.
Similarly, the
Standards on Youth Friendly Reproductive Health Services & Minimum Service Delivery Package on YFRH Services: Service Delivery Guideline, n.d.
explicitly prohibit age from consideration:
Any person male or female who can conceive or cause conception regardless of age or marital status is eligible for family planning services including family planning counseling and advice.
Based on these inclusions, Ethiopia is placed in the green category for this indicator. Policy documents directly recognize the rights of young people to receive FP services.
The
National Guideline for Family Planning Services in Ethiopia, 2020
includes language acknowledging the right to access FP services regardless of marital status:
Equity and non-discrimination: Individuals have the ability to access comprehensive contraceptive services free from discrimination, coercion and violence. FP services should not vary by non-medically indicated characteristics, such as age, geography, language, ethnicity, disability, HIV status, income, and marital or other status.
The guidelines also recognize the unique context of adolescents and youth seeking family planning and confirm that services need to be accessed regardless of marital status:
Unmarried and married youth may have different sexual, FP, and other SRH needs. FP services can create an opportunity to discuss STIs, HIV, GBV, and other SRH issues. Because of ignorance and psychological and emotional immaturity, adolescents and youths
compliance with the use of FP methods may not be optimal. In light of these facts, FP services need to be adolescent and youth-friendly and be accessible irrespective of their age and marital status. This implies services to be unbiased, non-discriminatory, affordable, confidential, convenient, and comprehensive.
Ethiopia is placed in the green category for this indicator because relevant policies directly support married and unmarried youth receiving FP services.
Ethiopian policies support youth
s access to a full range of FP methods regardless of age and marital status. The
Standards on Youth Friendly Reproductive Health Services & Minimum Service Delivery Package on YFRH Services: Service Delivery Guideline, n.d.
state as an objective:
[T]o enable youth [to] have access to a range of contraceptive methods and information so that they would be able to decide on when and how they would be able to have children and get protected from unplanned pregnancy.
The Standards further affirm youth access to all contraceptive methods:
Ensure availability and accessibility of all types of modern contraceptives, including LARC [long-acting and reversible contraceptives], for adolescents and youth who are sexually active.
The
National Guideline for Family Planning Services in Ethiopia, 2020
confirms that the provision of contraceptive methods follows the most recent medical eligibility criteria established by the World Health Organization, which allows adolescents and youth to access to a full range of contraceptive methods, including long-acting reversible contraceptives, regardless of age, marital status, or parity.
Ethiopia is placed in the green category for this indicator.
Although the availability of emergency contraception (EC) is not factored into the categorization of this indicator, it is worth noting that the policy environment in Ethiopia supports youth accessing EC. The
National Adolescent and Youth Health Strategy, 2016-2020
specifically mentions a priority intervention to distribute EC and the Standards also include it in the package of comprehensive sexual and reproductive health services to which youth should have access.
The
National Adolescent and Youth Health Strategy, 2016-2020
includes a priority intervention related to
comprehensive life skills, family life and sexuality education
and a related target to increase access to comprehensive sexuality education (CSE) to 62.5% of adolescents and youth by 2020. Noting weaknesses in CSE implementation to date, the strategy identifies priority actions that touch on some of the United Nations Population Fund (UNFPA) essential components of CSE, including reaching out-of-school and vulnerable youth. However, several of the UNFPA essential elements of CSE, such as an integrated focus on gender and ensuring scientifically accurate sexual and reproductive health information, are not addressed in these priority actions.
The
School Health Program Framework, 2017
provides further guidance on the provision of sexuality education. The Program Framework includes sexual and reproductive health as one of its 10 packages:
Package 6: Sexual and reproductive health (SRH) services
Access to SRH services is a primary concern of adolescent and youth due to the sensitive nature and risk of sex and sexuality issues. In this package, age appropriate SRH information and education will be provided at each level of school. The provision of SRH services will be comprehensive and rights-based. Comprehensive SRH rights state that services should be voluntary, informed and affordable.
The major focus of the SRH package will occur in the 2nd cycle education and will focus on sexual health education and health behavior promotion, including information on delaying and abstaining sexual activity.
. At the secondary school level, students seeking HIV testing and sexually active students seeking contraceptive services like condoms, oral contraceptives (including emergency contraception), injectables, and implants will be referred to the nearby health facility.
The Program Framework mentions all nine UNFPA essential components either as guiding principles or within activities, but is limited in the breadth of instruction regarding sexuality, sexual behavior, and reproductive health.
Like the National Adolescent and Youth Health Strategy, other policies suggest additional emphasis will be placed on educating Ethiopian youth regarding FP. The
Costed Implementation Plan for Family Planning in Ethiopia, 2015/16-2020
incorporates an activity that seeks to work through the Ministry of Education to strengthen sexuality education:
MC1.4 Advocate with the MOE [Ministry of Education] to assess the capacity of schools to integrate SRH and family planning into the curriculum, including sexual education in the school health programme.
Moreover, the
Education Sector Development Programme V, 2015/16-2019/20
proposes revising the school curriculum by integrating life skills to increase awareness of sexual education:
The revision will address the needs of both males and females and will integrate life skills to increase awareness of issues such as HIV/AIDS, sexual education and DSA [drug and substance abuse], to help all students to lead safe and healthy lives. The curriculum revision will also pay attention to co-curricular activities and structures, to improve linkages and efficiency in the delivery of life skills training through formal and informal channels.
Ethiopia is placed in the yellow category for this indicator. Policies directly support providing some form of sexuality education and indicate that the development of a more robust curriculum is a priority for the country.
The policy environment in Ethiopia strongly supports the provision of youth-friendly FP services. Multiple policies reviewed incorporate youth-friendly FP services.
The
National Reproductive Health Strategy, 2016-2020
discusses the need for services to be tailored to meet the needs of youth. The Strategy outlines strategic interventions to increase access to sexual and reproductive health (SRH) information, education, and services, including provider training:
- Train health workers on adolescent-friendly health care to improve skills on providing quality adolescent and youth-friendly SRH information and services.
- Train the HEWs [health extension workers] on providing appropriate SRH information and services as per the standard.
- Develop and distribute job-aids for health workers including HEWs in all health facilities
To comprehensively address the range of health issues faced by youth in Ethiopia, the Ministry of Health broadened the scope of the most recent adolescent health policy, the
National Adolescent and Youth Health Strategy, 2016-2020.
SRH remains a key feature in this policy, which seeks to increase contraceptive prevalence among youth, reduce unmet need for modern contraception, and reduce unintended adolescent pregnancy.
The
Standards on Youth Friendly Reproductive Health Services & Minimum Service Delivery Package on YFRH Services: Service Delivery Guideline, n.d.
detail specific aspects of youth-friendly service delivery that align with the three elements of service delivery:
SRH services for the youth should be provided at an affordable cost or for those who can not pay for free.
Provision of very essential services like counseling, pregnancy and HIV testing, dispensing of different contraceptive methods should be carried out as much as possible by a single service provider or in an arrangement that ensures the privacy of the youth client.
Health workers are trained to provide services in a non-judgmental and friendly way.
The
National Guideline on Family Planning Services in Ethiopia, 2020
outlines the country
s rights-based approach to service delivery, which refers to an individual
s right to exercise control over their body, sexuality, and reproduction, including
the right to privacy and confidentiality.
The guideline also outlines the minimum standards of quality family planning services, including ongoing training of health care personnel, provision of services without bias or judgment, ensuring privacy and confidentiality in both space and provider-client relationships, and provision of contraceptives at an accessible cost.
All three service delivery elements of adolescent-friendly contraceptive service provision are recognized in the policies reviewed. Thus, Ethiopia is placed in the green category for this indicator.
The importance of building community support for youth FP services features in the priority interventions of Ethiopia
National Adolescent and Youth Health Strategy, 2016-2020":
- Leverage existing community health structures to provide adolescent and youth health information and age appropriate CSE [comprehensive sexuality education]- utilize the Health Extension Program involving Health Extension Workers and Health Development Army.
- Undertake community-based initiatives for demand creation through peers, health extension workers, counselors and others.
- Strengthen and engage community-based forums and faith-based organizations, including religious institutions, one-to-five networks, and community support groups, in improving adolescent health.
- Strengthen community involvement in prevention of early and unintended pregnancy.
- Promote education of parents and the community on the health and rights of adolescents and youth.
The Health Strategy recognizes gender inequalities and includes related priority actions:
- Mainstream gender and address its concerns in all adolescent and youth health programs.
- Empower adolescents to challenge gender stereotypes, discrimination and violence within peers/families, educational institutions, workplaces and public spaces.
- Assess and identify key structural forces that affect health and drive disparities, including gender-related structural and institutional biases across sectors.
Community support for youth sexual and reproductive health is featured in other documents, including the
Standards on Youth Friendly Reproductive Health Services & Minimum Service Delivery Package on YFRH Services: Service Delivery Guideline, n.d.
Ethiopia is placed in the green category for this indicator, as the policy documents reviewed thoroughly address building community support for youth FP services and address gender norms.
As no law or policy exists that addresses parental or spousal consent for youth access to FP services, Guinea is placed in the gray category for this indicator.
The
Plan national de d
veloppement sanitaire, 2015-2024
aims to integrate youth sexual and reproductive health services into health facilities with a specific target to reduce experiences of stigmatization or judgment among youth:
80% des ado-jeunes utiliseront les services de sant
sexuelle et reproductive sans stigmatisation ni jugement
The
Plan d
action national budg
de planification familiale de la Guin
e, 2019-2023" also addresses the judgment that youth may experience from providers:
Deuxi
mement, l
offre de services de PF est inadapt
e aux jeunes. Le personnel soignant des centres ne sait pas comment les recevoir. On peut citer en exemple le manque de confidentialit
et m
me parfois des jugements s
res de la part du personnel des centres.
However, Guinea
s policy environment does not explicitly prohibit providers from exercising personal bias or discrimination. The
Normes et proc
dures en sant
de la reproduction, 2016
uses direct language when discussing the conduct of providers in HIV/AIDS screening, stating that providers must avoid stigmatization and discrimination. For Guinea to be placed in the green category, a definitive statement, similar to that provided for HIV/AIDS services, is needed that says providers may not use personal bias and discrimination against youth in FP services. Guinea is placed in the gray category for this indicator.
The
Loi portant la sant
de la reproduction, 2000
states that reproductive health is a right guaranteed to all individuals regardless of age:
Article 2: Caract
re universel du droit
la sant
de la reproduction
Tous les individus sont
gaux en droit et dignit
en mati
re de sant
de la reproduction. Le droit
la sant
de la reproduction est un droit universel fondamental garanti
tout
tre humain, tout au long de sa vie, en toute situation et en tout lieu. Aucun individu ne peut
tre priv
de ce droit dont il b
ficie sans discrimination aucune fond
e sur l'
ge, le sexe, la fortune, la religion, la situation matrimoniale ou sur toute autre consid
ration.
Further, the
Standards de services de sant
adapt
s aux adolescents et aux jeunes, 2013
state that youth have the right to quality health services regardless of age:
L
laboration des pr
sents standards de Services de Sant
Adapt
s aux Adolescents et Jeunes (SSAAJ) a
guid
e par les principes suivants:
Le respect des droits humains et en particulier le droit des adolescents/jeunes
s aux services de sant
de qualit
sans aucune discrimination li
leur
ge, sexe, religion ou condition sociale.
The
Standards de services
include contraception in the minimum package of services for adolescents and support youth access to these services regardless of age. Guinea is placed in the green category for this indicator.
The
Loi portant la sant
de la reproduction, 2000
states that reproductive health is a right guaranteed to all individuals regardless of marital status:
Article 2: Caract
re universel du droit
la sant
de la reproduction
Tous les individus sont
gaux en droit et dignit
en mati
re de sant
de la reproduction. Le droit
la sant
de la reproduction est un droit universel fondamental garanti
tout
tre humain, tout au long de sa vie, en toute situation et en tout lieu. Aucun individu ne peut
tre priv
de ce droit dont il b
ficie sans discrimination aucune fond
e sur l'
ge, le sexe, la fortune, la religion, la situation matrimoniale ou sur toute autre consid
ration.
This statement is somewhat contradicted by preceding language in the law that refers specifically to married couples when defining reproductive health:
Par Sant
de la Reproduction
elle suppose que toute personne se trouvant dans un lien de mariage peut mener une vie sexuelle satisfaisante en toute s
curit
, qu'elle est capable de procr
er en toute libert
. Cette derni
re condition implique d'une part que les conjoints ont le droit d'
tre inform
s et d'utiliser la m
thode de planification ainsi que d'autres m
thodes de planification non contraires
la loi.
Because the law extends access to FP services regardless of marital status, but places particular emphasis on the rights of married couples, it creates room for confusion in its applicability to unmarried youth. Therefore, Guinea is placed in the yellow category for this indicator.
The
Standards de services de sant
adapt
s aux adolescents et aux jeunes, 2013
outline the minimum package of services for adolescents, which states that all contraceptive methods should be available to youth. However, the
Standards de services
do not define all methods as including long-acting reversible contraceptives (LARCs).
The
Plan d
action national budg
de planification familiale de la Guin
e, 2019-2023" discusses targeting young people in the supply of FP services by expanding the range of methods, including scale-up of LARCs:
Objectif 2: Garantir la couverture en offre des services de PF EN [espacement des naissances] et acc
s aux services de qualit
en renfor
ant la capacit
des prestataires publics, priv
s et communautaires et en ciblant les jeunes des zones rurales et enclav
es avec l
largissement de la gamme des m
thodes, y compris la mise
chelle des MLDA [m
thodes
longue dur
action] et PFPP [planification familiale du post-partum], l
lioration des services et prestations adapt
s aux besoins des jeunes notamment dans les infirmeries scolaires et universitaires sans oublier la prise en charge de la PF int
e dans les autres services de SR [sant
reproductive] (PF postpartum, SAA [soins apr
s avortement], VIH, Vaccination, Fistules, Paludisme, etc
)
While the
Plan d'action
discusses providing LARCs to young people, Guinea
s policy environment does not require health providers to offer LARCs regardless of age. Therefore, Guinea is placed in the yellow category for this indicator.
In Guinea, access to information and education about sexual and reproductive health is a recognized right described in the
Loi portant la sant
de la reproduction, 2000
:
Article 4 : Droit
l'information et
l'
ducation
Tout individu, tout couple a le droit
l'information et
l'
ducation relatif aux risques li
la procr
ation et
l'efficacit
de toutes les m
thodes de r
gulation des naissances.
Several policies describe plans for introducing sexuality programming in schools. The
Plan d
action national budg
de planification familiale de la Guin
e, 2019-2023
includes the implementation of a comprehensive sexuality education (CSE) approach to improve young people
s knowledge of sexual and reproductive health :
A1. Mise en place d
une approche d
Education Compl
la Sexualit
(ECS) pour les jeunes scolaris
s et non/d
scolaris
s ou en situation de vuln
rabilit
.
Activit
:
- Produire un argumentaire en faveur de l
ducation compl
te des adolescents et des jeunes en collaboration avec les leaders religieux pour renforcer les modules compl
mentaires sur la SRAJ [sant
reproductive des adolescents et des jeunes]
int
grer dans l
enseignement des
ves par un consultant pendant 10 jours
- Faire un plaidoyer en direction du Secr
tariat d
Etat charg
des Affaires Religieuses, de l
Education Nationale, du MASEF [minist
re de l
Action Sociale, de l
Enfance et de la Famille] (MAPF ET L
ENFANCE), de la Soci
Civile et des Relations avec le Parlement et de la Jeunesse, etc., pour l
gration des modules des SRAJ dans les curricula de formation
-
laborer
et multiplier les supports
ducatifs (affiches, d
pliants, bo
image
) sur l
ducation compl
te cibl
e
- Adapter et traduire les modules pour une formation des adolescent(e)s et des jeunes non scolaris
s en arabe et 3 langues nationales
- Identifier et former 20 enseignants exp
riment
s pour assurer la formation des formateurs
- Animer 5 sessions de formation des enseignants
One of the essential CSE components is to reach youth in formal and informal settings. The
Feuille de route nationale pour acc
rer la r
duction de la mortalit
maternelle, n
onatale et infanto-juv
nile, 2012-2016
and the
Plan strat
gique en sant
et d
veloppement des adolescents et des jeunes en Guin
e, 2015-2019
describe plans to reach youth in and out of school with sexuality education, in addition to broader awareness campaigns to spread information on sexual and reproductive health.
Another essential component of CSE aims to strengthen youth advocacy and civic engagement. The
Plan strat
gique
emphasizes youth participation in designing and implementing health programs, but it does not include plans for teaching youth about youth advocacy and civic engagement within a CSE program.
Guinea
s policies do not describe specific components that should be included in a sexuality education program, with the exception of reaching youth in formal and informal settings. Therefore, Guinea is placed in the yellow category for this indicator.
Guinea
s policy environment is promising in its acknowledgement of the importance of health services tailored to youth, but it does not outline all three service-delivery elements of adolescent-friendly contraceptive services.
The
Standards de services de sant
adapt
s aux adolescents et aux jeunes, 2013
note that adolescents face provider discrimination when they seek sexual and reproductive health services. To remedy this, the Standards de services include a goal to ensure that providers are trained to offer youth-friendly services:
Tous les prestataires ont les connaissances, les comp
tences, et les attitudes positives (requises) pour offrir des services adapt
s aux besoins des adolescents et des jeunes.
The
Plan d
action national budg
de planification familiale de la Guin
e, 2019-2023
defines a specific target to increase provider capacity for youth-friendly FP services:
A2. Renforcement de l'enseignement de la PF dans les
coles et facult
s de formation en sant
-
laborer/adapter des manuels de formation en prise en charge des jeunes et des adolescents dans les FS [formation sanitaire] offrant la PF
- Identifier et
valuer la performance des OSC actives dans la lutte contre l
infection VIH/sida chez les jeunes et recenser chaque ann
e 20 FS appropri
es pour la prise en charge des adolescents et des jeunes
- Renforcer l
quipement des FS pour offrir des services aux adolescents et aux jeunes
- Am
nager les services (espace horaire, activit
s, etc.
) pour prendre en compte les besoins des jeunes
- Superviser les prestations offertes par les prestataires form
s
The
Normes et proc
dures en sant
de la reproduction, 2016
describe the procedures that providers should follow when attending to youth at each level of the health system. For example, the document encourages providers to listen attentively to youth. The
Plan strat
gique national de la sant
maternelle, du nouveau-n
, de l
enfant, de l
adolescent et des jeunes, 2016-2020
includes activities to strengthen the capacity of youth-friendly service providers and to combat the stigmatization that youth face when accessing services:
6.5: Sant
reproductive et sexuelle des adolescents et jeunes : Am
lioration de l
s des adolescents et jeunes
des services adapt
leurs besoins du point de vue sant
ducation, emploi et information...
Interventions :
Renforcement des capacit
s des prestataires en sant
et d
veloppement des adolescents et jeunes y compris la lutte contre la stigmatisation des ado/jeunes dans les structures
The
Standards de services
include a guiding principle on respect for the confidentiality and privacy of youth. However, Guinea
s policies do not adequately address the provision of no-cost or subsidized services. The
Standards de services
include an activity to make health products affordable to adolescents, but do not specifically address the cost of FP services. Therefore, Guinea is placed in the yellow category for this indicator.
One of the five overarching standards described in the
Standards de services de sant
adapt
s aux adolescents et aux jeunes, 2013
includes planned activities for mobilizing communities around youth-friendly services, which include contraceptive services:
Standard 4: La communaut
- y compris les adolescents et les jeunes - facilite la mise en place et l
utilisation des services de sant
adapt
s aux adolescents et aux jeunes.
- Les organisations
base communautaire les leaders communautaires, les enseignants, les agents communautaires/Assistants sociaux et les associations de jeunes sont mobilis
es autour des PPS [points de prestation de services] pour faciliter l
utilisation des services de sant
par les adolescents et les jeunes
- Les organisations
base communautaire, les leaders communautaires et les enseignants, les agents communautaires/Assistants sociaux et les associations de jeunes, sont orient
s en vue de faciliter l
utilisation des PPS par les A&J [les adolescents et les jeunes]
- Les leaders communautaires/parents encouragent les A&J
utiliser les SSAAJ
[services de sant
adapt
s aux adolescents et jeunes].
The
Plan strat
gique en sant
et d
veloppement des adolescents et des jeunes en Guin
e, 2015-2019
discusses building support in communities and addressing gender norms. However, this document is not specific to youth sexual and reproductive health services, and it does not describe youth access to contraception; it instead refers to youth health services in general. The
Standards de services
make brief mention of gender mainstreaming, but provide little detail.
Because Guinea
s policies outline a detailed strategy to build community support but do not have a detailed strategy for addressing gender norms in youth access to FP, the country is placed in the yellow category for this indicator.
In its description of the current sexual and reproductive health situation in Haiti, the "Plan strat
gique national de sant
sexuelle et reproductive, 2019-2023" notes that young people and adolescents under age 18 have limited access to health services without parental permission. The
Plan strat
gique
does not specify whether this limited access is due to an unsupportive policy environment or a sociocultural environment. In the absence of clarity within policies around parental consent and with no mention of spousal consent, Haiti is placed in the gray category for this indicator.
The
Manuel de normes en planification familiale et en soins maternels, 2009
establishes the right of everyone, including adolescents and young people, to use the contraceptive method of their choice from a full range of available methods and with no influence from the provider. The
Manuel de normes
also notes that providers should create an environment that allows clients to safely express their needs:
MENT I : CHOIX DE LA M
THODE
Le client doit pouvoir obtenir la m
thode de son choix. Aussi, l
Institution doit veiller
ce qu
il n
y ait pas de biais au niveau de l
offre des m
thodes pour ne pas influencer le choix du client. De plus, l
Institution doit assurer la disponibilit
une grande gamme de m
thodes pour faciliter et satisfaire le choix du client, puisque les besoins de m
thode sp
cifique varient avec l
ge, le statut matrimonial, la parit
de la femme et le sexe.
ELEMENT IV
: RELATIONS INTER-PERSONNELLES
: CLIENT / PRESTATAIRE.
Des relations empreintes de cordialit
entre le personnel et le client comptent beaucoup pour induire la satisfaction du client. Que ce soit au niveau de l
accueil pour l
inscription et l
enregistrement, que ce soit lors du Counseling ou de l
examen clinique, le personnel doit faire preuve d
empathie, de respect pour le client. L
environnement de la consultation doit pr
senter un cachet d
intimit
et de confidentialit
. Le client doit
tre mis en confiance pour l
inciter
exprimer sans r
serve ses besoins.
Although the
Manuel de norms
notes that health facilities should not allow bias to interfere with method choice, it does not clearly state that providers must authorize medically advised FP services to youth without personal bias or discrimination. Haiti is place in the yellow category for this indicator.
The
Manuel de normes en planification familiale et en soins maternels, 2009" includes women of reproductive age who are sexually active as well as young people with sexual health and reproductive health needs as beneficiaries of family planning services:
Les b
ficiaires des services sont :
1) Les couples qui d
sirent
tre inform
s en mati
re de planification familiale ou la pratiquer.
2) Les femmes qui ont des besoins en Sant
de la Reproduction et sexuelle.
3) Les femmes en
ge de procr
er sexuellement actives et qui veulent
viter une grossesse non d
e, ou qui cherchent
espacer leurs grossesses et qui sont donc
la recherche d
une m
thode d
espacement des naissances.
4) Les hommes en
ge de procr
er qui veulent assurer eux-m
mes ou partager avec leur partenaire la responsabilit
du contr
le des naissances, soit en choisissant une m
thode masculine, soit en encourageant leur partenaire
choisir et
utiliser une m
thode contraceptive efficace.
5) Les hommes et les femmes qui ne veulent plus avoir d
enfants et qui optent pour une m
thode d
finitive de contraception chirurgicale.
6) Les jeunes qui ont des besoins en sant
sexuelle et en Sant
de la Reproduction.
7) Les couples qui ont besoin de procr
ation.
As the
Manuel de normes
supports youth access to family planning, Haiti is placed in the green category for this indicator.
The
Plan strat
gique national de sant
sexuelle et reproductive, 2019
2023
includes a multisectoral strategy to improve the legal framework to support young people in sexual and reproductive health services. However, as no current policy could be identified that supported youth access to FP services regardless of marital status, Haiti is placed in the gray category for this indicator.
The
Manuel de normes en planification familiale et en soins maternels, 2009
includes young people as beneficiaries to family planning services:
Les b
ficiaires des services sont :
6) Les jeunes qui ont des besoins en sant
sexuelle et en Sant
de la Reproduction.
The
Manuel de normes
further states that clients must be able to select methods of their choice, noting that health facilities should ensure a wide range of methods to facilitate client choice:
MENT I : CHOIX DE LA M
THODE Le client doit pouvoir obtenir la m
thode de son choix. Aussi, l
Institution doit veiller
ce qu
il n
y ait pas de biais au niveau de l
offre des m
thodes pour ne pas influencer le choix du client. De plus, l
Institution doit assurer la disponibilit
une grande gamme de m
thodes pour faciliter et satisfaire le choix du client, puisque les besoins de m
thode sp
cifique varient avec l
ge, le statut matrimonial, la parit
de la femme et le sexe.
The
Manuel de normes" continues to outline all available methods, including notes on how they work, their efficacy, and advantages and disadvantages, including side effects, eligibility, and limitations. As Haitian policy documents include young people as beneficiaries to family planning and support their access to a range of methods, including long-acting reversible contraceptives, Haiti is placed in the green category for this indicator.
Although the availability of emergency contraception (EC)
is not factored into the categorization of this indicator, note that the
Manuel de normes
also includes EC in the list of methods.
The "Plan strat
gique national de sant
des jeunes et adolescents, 2014-2017" lists the development of a sexuality education curriculum by the Ministry of Education and Vocational Training as an opportunity to support youth health. The
Plan strat
gique
includes an objective to empower young people to be responsible in their sexual behavior and outlines multiple interventions around sexuality education in formal and informal settings:
4.4 Habiliter les jeunes
une sexualit
responsable. Interventions
4.4.1 Appui au MENFP [minist
re de l
ducation nationale et de la formation professionnelle] pour l
implantation d
un programme d
ducation sexuelle dans les
coles.
4.4.2 Formation/recyclage de trois formateurs de pairs
ducateurs par section communale en partenariat avec les ONG [organisations non gouvernementales]
uvrant dans le domaine de la sant
des jeunes et des adolescents.
4.4.3 Recensement des organisations de jeunes.
4.4.4 Formations des jeunes par les pairs
ducateurs au niveau des associations, groupements de jeunes et autres initiatives de jeunes.
4.4.5 Implantation d
une ligne t
phonique d
informations sant
jeunes et adolescent.
4.4.6 Diffusion d
informations sant
et sant
sexuelle des jeunes sur un r
seau social (FACE Book).
4.4.7 Diffusion d
informations dans le cadre de l
organisation de Journ
es r
atives et de grandes mobilisations de jeunes et d
adolescents.
4.4.8 C
bration de la Journ
e internationale de la jeunesse.
The "Plan strat
gique national de sant
sexuelle et reproductive, 2019-2023" aims to strengthen the knowledge of young people ages 10 to 24 on the topic of sexual health. Intervention activities include strengthening the existing sex education program in schools:
Activit
s :
- D
velopper une strat
gie de communication sur la sexualit
et le droit des jeunes.
- Renforcer la formation des ASCP [agent de sant
communautaire polyvalent] sur la sant
des adolescents et des jeunes.
- Renforcer les capacit
s des professeurs
transmettre aux jeunes et adolescents dans les
coles, le programme d'
ducation sexuelle existant.
While both policies provide approaches to implementing sexuality education in and out of school, no comprehensive sexuality education framework (CSE) could be located, nor do available policies describe the nine essential components of a CSE program as defined by the United Nations Population Fund (UNFPA). Haiti is placed in the yellow category for this indicator.
To support its objective to reduce the number of unwanted pregnancies among youth ages 15 to 24, the "Plan strat
gique national de sant
sexuelle et reproductive, 2019-2023" aims to implement a youth-friendly pilot project in three public institutions. The three institutions will adapt international standards for quality, comprehensive care for adolescents and young people, and the essential package of services as set by the World Health Organization:
STRAT
GIE 5.2.2
a) Mettre en
uvre dans au moins trois institutions de sant
les normes mondiales de l'OMS [Organisation mondiale de la sant
] et de l'ONUSIDA [Programme commun des Nations Unies sur le VIH / sida] pour la qualit
des services de sant
complets destin
s aux adolescents et adapt
s au contexte d'Ha
ti en tenant compte du paquet essentiel de services pour les jeunes de 15
24 ans.
Activit
s :
Adapter les standards internationaux pour des soins de sant
complets de qualit
destin
s aux adolescents et jeunes de 15
24 ans.
Mettre en
uvre ces standards dans trois institutions publiques du pays dans le cadre d'un projet pilote.
valuer l'am
lioration de la qualit
des soins complets pour adolescents au terme du projet pilote.
tendre le projet pilote
d'autres institutions
partir des r
sultats obtenus dans l'
valuation
The "Plan strat
gique national de sant
des jeunes et adolescents, 2014-2017" includes objectives and specific interventions to strengthen the health system structure by improving the quality of services for adolescents and young people. The specific interventions promote privacy and confidentiality of services as well as provider training:
2.3 Renforcer progressivement les d
partements sanitaires pour faciliter un fonctionnement ad
quat des services de sant
offerts aux jeunes et aux adolescents.
Interventions
...
2.3.2 Am
nagement de salles d
accueil et de consultation amis des jeunes, refl
tant un aspect convivial pour les jeunes.
2.3.3 Atelier de sensibilisation des responsables d
partementaux
lioration du programme de sant
des jeunes.
2.3.4 Formation de prestataires formateurs de jeunes
2.3. 6 Plaidoyer pour l
gration d
activit
s SS/SR [sant
sexuelle / sant
reproductive] des jeunes dans les budgets d
partementaux.
2.3.7 Elaboration d
un plan op
rationnel SJA [sant
des jeunes et des adolescents] dans chaque d
partement.
2.4 Rendre accessible une prise en charge normalis
e, int
e et holistique aux jeunes et aux adolescents.
Interventions
2.4.1 Sp
cification du Paquet essentiel de services institutionnels aux jeunes et adolescents.
2.4.6 Approvisionnement des points de services locaux et des organisations de jeunes en intrants SS/SR/PF et autres m
dicaments pour les jeunes
2.4.8 Acquisition de mat
riels, fournitures et
quipements audiovisuels pour les espaces de services aux jeunes
2.4.11 Mise en place de consultations gyn
cologiques sp
cifiques accessibles aux jeunes au niveau des [h
pital communautaire de r
rence].
The
Plan strat
gique national de sant
des jeunes et adolescents
objective to establish effective communication between young people and providers includes additional activities to train providers to be more holistic in their care:
4.2
tablir des liens efficaces de communication entre jeunes et prestataires des institutions publiques de sant
. Interventions
4.2.1 Formation des prestataires en
ducation sexuelle, sant
sexuelle, prise en charge holistique des jeunes, suivi des interventions visant les jeunes, initiation
usage des supports
ducatifs.
4.2.2 R
union de sensibilisation sur les droits sexuels des jeunes et des adolescents.
The
Plan strat
gique national de sant
des jeunes et adolescents
also notes that interviews with stakeholders revealed that program officials overwhelmingly said health care providers were currently unable to welcome young people without discrimination, and they identified education and training as key to improving the state of youth services.
The
Manuel de normes en planification familiale et en soins maternels, 2009,
which names youth as beneficiaries to family planning services, clearly states that family planning services are free:
1.6. COUT DES SERVICES
Les services de PF sont totalement gratuits.
The
Manuel de normes
emphasizes the importance of provider attitudes and states that providers must provide privacy and confidentiality for all clients:
ELEMENT IV : RELATIONS INTER-PERSONNELLES: CLIENT / PRESTATAIRE. Des relations empreintes de cordialit
entre le personnel et le client comptent beaucoup pour induire la satisfaction du client. Que ce soit au niveau de l
accueil pour l
inscription et l
enregistrement, que ce soit lors du Counseling ou de l
examen clinique, le personnel doit faire preuve d
empathie, de respect pour le client. L
environnement de la consultation doit pr
senter un cachet d
intimit
et de confidentialit
. Le client doit
tre mis en confiance pour l
inciter
exprimer sans r
serve ses besoins.
Haiti
s policies specifically reference providing FP services as part of a package of services and include the three service-delivery elements: provider training, enforcing confidentiality and privacy, and providing no-cost or subsidized services. Haiti is placed in the green category for this indicator.
The "Plan strat
gique national de sant
des jeunes et adolescents, 2014-2017" includes an objective to promote favorable behaviors for young people
s health. The objective
s detailed activities include the establishment of partnerships between parents and churches so parents gain a better understanding of how they can share information on sexuality education with their children and a community forum to sensitize parents to their roles in their child
s sexual health. The objective also includes a meeting of community leaders to engage them in promoting an enabling environment for adolescent sexual health:
4.1 Am
liorer la communication enfant-parents, en mati
re de sant
en g
ral et de sant
sexuelle en particulier, au niveau de toutes les sections communales du pays.
4.1.5 Organisation de r
unions avec les leaders communautaires pour les engager dans des actions visant la promotion, la protection de la sant
et de la sant
sexuelle des adolescents et des jeunes.
The
Plan strat
gique national de sant
des jeunes et adolescents
builds further support for youth FP by including multiple activities with which to engage the community to promote adolescent and youth sexual health:
4.3.1 Organisation de r
unions avec les leaders communautaires pour les engager dans des actions visant la promotion et la protection de la sant
, de la sant
sexuelle des adolescents et des jeunes.
4.3.2 Sensibilisation des communaut
s lors de festivit
s patronales, foires et autres activit
s communautaires de masse et les engager dans des actions visant la promotion et la protection de la sant
, de la sant
sexuelle des adolescents et des jeunes.
4.3. Diffusion de spots de sensibilisation
la radio pour inciter les communaut
s et susciter leur int
engager dans des actions visant la promotion et la protection de la sant
, de la sant
sexuelle des adolescents et des jeunes.
The
Plan strat
gique national de sant
des jeunes et adolescents
falls short of outlining a full gender strategy for youth family planning, but does include an activity on raising awareness for gender equity among providers of public health:
4.2
tablir des liens efficaces de communication entre jeunes et prestataires des institutions publiques de sant
.
4.2.3
Promotion et sensibilisation pour l
quit
de genre et pr
vention de la violence.
The "Plan strat
gique national de sant
sexuelle et reproductive, 2019-2023" also links service delivery with activities that build support for FP in communities:
Mobiliser la soci
civile, les
lus locaux, les collectivit
s territoriales autour d'un plan efficace de promotion de la sant
sexuelle et reproductive et des droits des femmes et des filles
labore et mis en
uvre conjointement avec les institutions de sant
.
Activit
:
Mobiliser les institutions de sant
pour la mise en place de strat
gies et plans de communication et de sensibilisation au niveau communautaire en SSR et droits des femmes et des filles, conjointement avec la soci
civile, les
lus locaux, et les collectivit
s territoriales.
Soutenir l'implication des communaut
s, groupes de femmes,
lus locaux, collectivit
s territoriales dans l'organisation et la gestion des services communautaires et institutionnels de sant
sexuelle et reproductive, dans une optique de renforcement de la qualit
des services.
Initier de nouveaux mod
les d'intervention en SSR aupr
s des hommes, tant au niveau communautaire qu'institutionnel.
The
Plan strat
gique national de sant
sexuelle et reproductive
also outlines a strategy to target parents as key factors in establishing a more favorable sexual and reproductive health environment for young people ages 10 to 24, including training parents on their role in supporting FP information and involving community organizations to promote and protect youth reproductive health needs:
Favoriser la mise en place de programmes de formation et de sensibilisation des parents sur le r
le qu'ils ont
jouer aupr
s de leurs enfants dans le domaine de l'
ducation
la sant
, de l'
ducation sexuelle et la n
cessit
de partager avec leurs enfants les informations, exp
riences et valeurs en mati
re de sexualit
Encourager l'implication des organisations communautaires et conseils communaux dans des actions visant la promotion, la protection de la sant
et de la sant
sexuelle des jeunes et des adolescents.
The policies reviewed outline the need to build a supportive social environment for youth FP through engagement of families and communities; however, they fall short of adequately addressing gender norms as they relate to youth access to FP. Haiti is placed in the yellow category for this indicator.
No law or policy in India explicitly addresses consent from a third party to access to FP services. India is therefore placed in the gray category for this indicator.
The
Reference Manual for Doctors: Contraceptive Updates, 2005
provides medical eligibility checklists for each contraceptive method.
The
Rashtriya Kishor Swasthya Karyakram Operational Framework: Translating Strategy into Programmes, 2014
notes that that providers should ideally provide non-judgmental services:
2.10 The quality of counselling services will largely depend on the knowledge, attitude and skills of a counsellor. And in this context, the selection of Counsellors is important. Counsellors should ideally be:
- Non-judgmental, with a progressive attitude i.e. in no circumstances, should the counsellor try to impose his or her values
However, India
s policies do not directly require providers to provide medically advised FP services without personal bias and discrimination. Therefore, India is placed in the gray category for this indicator.
The
Reference Manual for Doctors: Contraceptive Updates, 2005
confirms youth access to FP services regardless of age:
In general, adolescents are eligible to use any method of contraception and must have access to a variety of contraceptive choices. Age alone does not constitute a medical reason for denying any method to adolescents, although sterilization is rarely appropriate for this age group. While some concerns have been expressed regarding the use of certain contraceptive methods in adolescents, (e.g., the use of progestogen-only injectables by those below 18 years), these concerns must be balanced against the advantages of avoiding pregnancy and existing guidelines be adhered to. It is clear that many of the same issues regarding appropriate contraceptive use that apply to older clients apply to young people.
Since youth have access to all contraceptive methods regardless of age, India is placed in the green category for this indicator.
Multiple strategy documents discuss contraceptive provision to unmarried adolescents. In
A Strategic Approach to Reproductive, Maternal, Newborn, Child and Adolescent Health in India, 2013,
the section on adolescent-friendly health services confirms the availability of services to unmarried youth:
Services in adolescent health clinics will be available to all adolescents: married and unmarried, girls and boys, and will be further strengthened. Special focus will be given to establishing linkages with Integrated Counselling and Testing Centres (ICTCs) and making appropriate referrals for HIV testing and RTI/STI [reproductive tract infection/sexually transmitted infection] management; providing comprehensive abortion care; and provision of information, counselling and services for contraception to both married and unmarried adolescents.
The
Implementation Guide on RCH II Adolescent Reproductive Sexual Health Strategy, 2006
includes unmarried men and women as the target group for contraceptives and condom programming in primary health centers and district hospitals. The implementation guide further details the service delivery package for adolescents, which specifics unmarried youth:
SECTION ONE: SERVICE DELIVERY PACKAGE
STANDARD: Health facilities provide specified package of services that adolescents need
Services are to be made available for all adolescents, married and unmarried, girls and boys. Focus is to be given to the vulnerable and marginalized sub-groups. The package of services is to include promotive, preventive, curative and referral services. A plan of service provision as per the level of care may be developed based on the RCH II
[Reproductive and Child Health Phase II] service delivery plan presented in the previous section.
With the policy recognition that unmarried youth deserve access to contraception, India is placed in the green category for this indicator.
The
Reference Manual for Doctors: Contraceptive Updates, 2005
states that
adolescents are eligible to use any method of contraception and must have access to a variety of contraceptive choices.
Moreover, according to the
Facilitator
s Guide: Training Manual for Medical Officers, n.d.,
healthy adolescents are medically eligible to use all currently available methods of contraception.
Multiple reference manuals and guides identify contraceptive methods available in India and who can and cannot use them, acknowledging that some long-acting reversible methods may not be recommended as a first choice for certain age groups.
The "Reference Manual for Doctors" and the "Facilitator
s Guide: Training Manual for Medical Officers" both acknowledge that age is not a medical reason to withhold any contraceptive method, but it should be considered before providing either of two methods to youth of certain ages. The Training Manual includes the following guidance:
Tips for Facilitators
Age does not constitute a medical reason for withholding the provision of any method. However
age is a factor to be taken into account when considering the use of three methods:
- Progestin-only injectables (such as Depomedroxy Progesterone Acetate (DMPA), and Norethisterone Enanthate (NET-EN)) are not the first method of choice for those under 18, as there is a theoretical concern that bone development could be hindered.
- Intra-Uterine Contraceptive Devices (IUCD) are not the first method of choice for those under 20, as the risk of expulsion is higher in young, nulliparous women. Infection may lead to infertility as well.
The
Reference Manual for Injectable Contraceptive (DMPA), 2016,
however, states that progestin-only injectables are safe for women of any age, including adolescents.
Further, one of the strategies to reduce adolescent pregnancy in the
Rashtriya Kishor Swasthya Karyakram Strategy Handbook, 2014
includes access to long-acting reversible contraceptives (LARCs):
Referral for clinical contraceptives such intra-uterine contraceptive devices as per the protocol.
While many policy documents include medical eligibility criteria that has been adapted from the World Health Organization medical eligibility criteria, they do not explicitly mention youth
s right to access a full range of contraceptive services, including LARCs, regardless of marital status or parity. India is placed in the yellow category for this indicator.
Although the availability of emergency contraception (EC) is not factored into the categorization of this indicator, the
Implementation Guide on RCH II Adolescent Reproductive Sexual Health Strategy, 2006
explicitly states that adolescents may have access to emergency contraception without prescription, while the
Guidelines for Administration of Emergency Contraceptive Pills by Health Care Providers, 2008
confirm that EC should be provided to clients within their reproductive years regardless of their age and marital status.
The
Rashtriya Kishor Swasthya Karyakram Strategy Handbook, 2014
identifies the inclusion of family life education and life skills in school curricula as a community-level activity to support adolescent sexual and reproductive health (SRH). The
Strategy Handbook
also acknowledges the importance of peer educators to the strategy
s community approach; peer educators will be trained by teachers to share SRH information and lead discussions in and out of school settings.
The
Operational Guidelines on School Health Programme under Ayushman Bharat, 2018
aims to provide age-appropriate information about health and nutrition in schools, promote healthy behaviors, and create appropriate referrals to health centers and hospitals. However, the Operational Guidelines do not provide further detail on sexuality education beyond noting that SRH is age-appropriate health information for high school-aged students.
The
Adolescence Education Programme Life Skills Development: Facilitator
s Guide, n.d.
aims to support the development of positive behaviors to empower young people to make healthy choices and gain life skills. To reach these goals, the Education Programme outlines five objectives:
- All schools provide accurate age-appropriate life skills based adolescence education in a sustained manner to young people (10-18 yrs) in schools;
- Every child is equipped with accurate information, knowledge and life skills to protect themselves from HIV and manage adolescent reproductive sexual health (ARSH) issues and concerns;
- All out-of-school adolescents are provided basic information and services on adolescent reproductive and sexual health, HIV prevention and prevention of substance abuse
- Effective integration of adolescence education components in school curriculum as well as the teacher education course takes place; and
- Linkages to youth friendly services are established and resources for additional information are easily
The Education Programme consists of three components, including
Process of Growing Up,
which covers topics of self-identity, gender roles, addressing myths and misconceptions, and links to youth-friendly services. It also includes peer educators who will be used as support for teachers in informal settings.
As outlined in the
Training and Resource Materials: Adolescence Education Programme [AEP], 2013,
the AEP has an integrated focus on gender and includes components that focus on understanding issues of discrimination and violations. The guiding principles of the Training and Resource Materials emphasize providing accurate and age-appropriate information to adolescents. They also include a peer education component, reaching youth engaged in both informal and organized education activities, thus touching on many of the essential United Nations Population Fund (UNFPA) components for CSE:
Objective 2. To enable adolescents to be aware of implications of child marriage adolescent pregnancy/parenting.
Objective 4. To empower adolescents to understand and challenge existing norms and inequalities related to gender and sexuality
Objective 5. To enable young people to understand various kinds of discrimination and violations and develop skills to counter/seek redressal
The
Reproductive, Maternal, Newborn, Child and Adolescent Health (RMNCH+A) Strategy, 2013
seeks to implement life skills education in educational institutions and community settings but does not specifically address education in the context of youth FP.
Since India
s policy environment supports SRH education but does not address all nine essential UNFPA components for CSE, India is placed in the yellow category for this indicator.
The
Implementation Guide on RCH II Adolescent Reproductive Sexual Health Strategy, 2006
lays out standards to guide implementation of adolescent sexual and reproductive health (SRH) interventions, including a standard for service providers to be sensitive to adolescents
needs:
Due to a variety of reasons, e.g. judgmental attitudes of service providers, many adolescents do not seek health services. Services providers are to be technically competent and motivated to provide services to adolescents as per their need/s. This standard seeks to ensure that the service providers imbibe and demonstrate appropriate attitudes and behaviour to reassure the adolescents in addressing their needs. The standard therefore seeks to address issues relating to service providers attitudes and motivation.
The Implementation Guide also outlines a training to build providers
capacity to provide services to adolescents without being judgmental, and covers topics related to contraception, pregnancy, and SRH:
The key contents of training are as follows:
- Adolescent growth and development
- Communicating with adolescents
- Adolescent Friendly Reproductive and Health Services
- Sexual and reproductive health concerns of boys and girls
- Nutrition and Anaemia in adolescents
- Pregnancy and unsafe abortions in adolescents
- Contraception for adolescents
- RTIs/STIs [reproductive tract infection/sexually transmitted infections] and HIV/AIDS in adolescents
It also includes a standard to build a conducive environment at health facilities that ensures confidentiality and audio/visual privacy:
- Clinic rooms must have window curtains and a bed-screen surrounding the examination table.
- It is advisable to... give clear instructions to the staff about not allowing any one into the clinic when a client is already there, in order to ensure privacy.
- The confidentiality policy of the clinic may be displayed and clearly expressed to the client in the first session itself.
- Client records to be kept out of reach of unauthorized persons.
The
Rashtriya Kishor Swasthya Karyakra Operational Framework: Translating Strategy into Programmes , 2014
outlines the role and recruitment of health counselors, and notes that counselors should be able to maintain privacy and confidentiality and withhold judgment. Similarly, the operational framework outlines the infrastructure for an adolescent-friendly health clinic (AFHC), and notes the following benchmarks:
Exhibit 2.04: Benchmarks for an AFHC
- Infrastructure clean, bright and colorful
- Can be easily accessed by the adolescents (distance, convenient working hours and cost)
- Adolescents are aware about the clinic and range of service it provides
- Non judgmental and competent health service providers
- Maintains privacy and confidentiality
- Community members are aware of the services provided and understand the need for the same
Both the Rashtriya Kishor Swasthya Karyakra
s operational framework and implementation guidelines include trainings for health care workers, counselors, and peer educators on adolescent-friendly health services but do not provide details on the trainings.
A Strategic Approach to Reproductive, Maternal, Newborn, Child and Adolescent Health in India, 2013
states that family planning commodities and services are provided free to every client during community-based doorstep distribution through accredited social health activists. It also acknowledges that adolescents in need of secondary and tertiary care will be entitled to
free treatment through Rastriya Swasthya Bima Yojona or State Health Insurance Scene.
The
National Population Policy, 2000
supports free supply of contraceptives in its operational strategy to implement a one-stop integrated and coordinated service-delivery package for basic health care and family planning in the community.
Since India
s policy environment includes all three service-delivery elements for youth-friendly contraceptive services, India is placed in the green category for this indicator.
The
Implementation Guide on RCH II Adolescent Reproductive Sexual Health Strategy, 2006
seeks to create an enabling environment in the community for adolescents
access to sexual and reproductive health (SRH) services by planning activities targeting key stakeholders such as community leaders, parents, teachers, and community-based organizations:
District programme managers are to ensure that steps are taken to help key stakeholders in the community to understand and respond to adolescent needs. Key audiences are to be identified whose support would be needed for creating an enabling environment within the community. Key stakeholders can include policy makers, administrators, community leaders, service providers, parents, teachers, community-based organizations, NGOs and the media.
The community can be engaged in a variety of ways, like seeking their views, providing information, and involving them in prioritizing areas for quality improvement. They can help to publicise and generate demand for high quality services and increase adolescents
use of them. Linkages may be established with community-based organizations, NGOs [nongovernmental organizations], private practitioners, social marketing and franchising outlets. Media can be effectively engaged in generating awareness about adolescent issues and their importance as well as spreading information about Adolescent Friendly Reproductive and Sexual Health Services. Mass media as well as folk media can be used judiciously
The
Implementation Guide on RCH II Adolescent Reproductive Sexual Health Strategy, 2006
also lays out activities that the district health officer can take to build a supportive environment for youth SRH, including orientation days to raise awareness on adolescent SRH issues and meetings to build support of unmarried adolescents
service use. The strategy acknowledges that building support requires continuous action:
- Efforts must be made to increase awareness of the community regarding the adolescent needs and how to respond to them.
- Adolescents must be encouraged by the community to access the services.
- Health functionaries organize meetings with other departments and the community at various levels of administration to emphasize the need and role of adolescent-friendly services
- Adolescent health issues to be discussed continuously in routine contacts with the community members.
Moreover, the Implementation Guide aims to give special attention to
gender and equity differentials at every stage of implementation.
It details a list of actions, which includes communication activities at the local level that address gender norms and the prevention of unwanted pregnancy.
The
Rashtriya Kishor Swasthya Karyakram Strategy Handbook, 2014,
under the SRH strategic priority to reduce adolescent pregnancy, includes a strategy and related interventions to address social pressures and cultural norms related to early marriage, conception, and contraception:
Strategies
Address social pressure and concerns related to early marriage, conception and contraception.
.
Interventions
Communication with individuals, families and communities, including men, to create support and influence cultural norms to reduce early marriage (such as information on the legal status of early marriage) and pregnancy.
Moreover, the
Rashtriya Kishor Swasthya Karyakram Operational Framework: Translating Strategy into Programmes, 2014
aims to increase awareness among parents, teachers, families, and other stakeholders about adolescent health needs, including SRH, through adolescent health days organized at a village level. While building support for FP services is not directly outlined as part of the content for adolescent health days, one stated purpose is to increase knowledge of and referrals to adolescent-friendly health centers that provide contraceptives.
A Strategic Approach to Reproductive, Maternal, Newborn, Child and Adolescent Health in India, 2013
acknowledges the special attention that should be given to community participation and notes that community structures should be mobilized through advocacy and capacity-building to create a conducive environment for utilization of available health services. However, the recommended process focuses on implementing accountability mechanisms and using community events as a platform for service outreach. The strategy mentions focused messaging to community members but without a specific focus on supporting youth FP:
In order to reduce adolescent pregnancy, focused messaging to individuals, families and communities (including men) will be reinforced through the Life Skills Education sessions that are delivered from various adolescent centric platforms including community outreach sessions and Anganwadi centres.
In addition, the Strategic Approach also refers to the Saksham scheme, which aims to empower boys by educating them on gender sensitivity:
Saksham aims to target young boys, in the age group 10
18 years, for their holistic development by giving lessons in gender sensitivity and inculcating in them respect for women.
While India
s policies outline strategies to build community support for youth SRH and address gender norms, they do not specifically address youth FP. India is placed in the yellow category for this indicator.
Despite Kenya
s strong policy environment supporting sexual and reproductive health (SRH) services for adolescents and youth, the legal stance on parental and spousal consent for youth accessing FP services remains noticeably weak.
The
Children Act, No. 8 of 2001, Revised Edition, 2019
which defines a child as anyone under age 18, does not specifically outline when parental consent is required but notes that a child
s right to health care is the responsibility of the parent:
- Right to Health Care
Every child shall have a right to health and medical care the provision of which shall be the responsibility of the parents and the government.
The
National Guidelines for Provision of Adolescent and Youth Friendly Services in Kenya, 2016
outline a clear strategy to improve adolescents
access to and use of SRH services. While this document identifies laws and policies requiring parental and partner approval as a structural barrier to youth accessing SRH services, it does not make any definitive statement on the right of adolescents to access services without parental and spousal consent.
Kenya is placed in the gray category for parental or spousal consent since no law or policy exists that addresses consent from a third party for youth to access FP services. The country could move into the green category for the indicator if policymakers pass a new policy with a provision that recognizes youth
s right to access FP services without parental or spousal consent.
Explicit policy language directs providers to offer nondiscriminatory, unbiased care to adolescents based on medical eligibility criteria. The
National Guidelines for Provision of Adolescent and Youth Friendly Services in Kenya, 2016
promote five characteristics of adolescent service provision that follow the World Health Organization
s Quality of Care framework for adolescent service provision: accessible, acceptable, appropriate, equitable, and effective. The National Guidelines specifically address the role of the provider to offer adolescent-friendly health services, including the provision of contraception, in a manner that respects the five quality of care characteristics:
The service providers should be non-judgmental and considerate in their dealings with adolescents and youth and deliver the services in the right way.
Kenya is placed in the green category for this indicator
as policies direct providers to deliver nonjudgmental FP services.
The right to health services, including reproductive health services, is recognized at the highest policy level in Kenya. The
Constitution of Kenya, 2010
recognizes the right of all people to access reproductive health care:
Article 43: (1) Every person has the right
(a) to the highest attainable standard of health, which includes the right to health care services, including reproductive health care.
The
Health Act, 2017
includes the right of people of reproductive age to access FP services:
Article 6: (1) Every person has a right to reproductive health care which includes
(a) the right of men and women of reproductive age to be informed about, and to have access to reproductive health services including to safe, effective, affordable and acceptable family planning services.
This strong declaration in favor of all people accessing health care sets the stage for equal access to health care services.
The
National Guidelines for Provision of Adolescent and Youth Friendly Services in Kenya, 2016
recognize adolescents
right to access services independent of their age, including FP and contraceptive services as a subset of services under the
Minimum Initial Service Package (MISP) for Reproductive Health.
Under the MISP operational guidelines, health providers are directed as follows:
Health staff should be aware that adolescents requesting contraceptives have a right to receive these services, regardless of age or marital status.
This explicit recognition of adolescents
right to contraception regardless of age is a critical step toward addressing the barriers many youth encounter when trying to access these services. Kenya is placed in the green category for this indicator.
The
National Guidelines for Provision of Adolescent and Youth Friendly Services in Kenya, 2016
recognize adolescents
right to access services independent of their marital status, including FP and contraceptive services as a subset of services under the
Minimum Initial Service Package (MISP) for Reproductive Health.
Under the MISP operational guidelines, health providers are directed as follows:
Health staff should be aware that adolescents requesting contraceptives have a right to receive these services, regardless of age or marital status.
Kenya is placed in the green category for this indicator as the policy environment includes a clear provision for youth to access FP services regardless of marital status.
Adolescents and youth in Kenya can access a full range of contraception under existing policies. The
National Guidelines for Provision of Adolescent and Youth Friendly Services in Kenya, 2016
include contraception as a component in the essential package of service offerings for adolescents:
Contraception counselling and provision of full range of contraceptive methods, including long-acting reversible methods.
While the
National Family Planning Guidelines for Service Providers, 6th Edition, 2016
support adolescent and youth access to all methods of contraception alongside counseling, it discourages the use of permanent methods:
Adolescents and youth in need of contraceptive services can safely use any method, following the guidelines and MEC [medical eligibility criteria] criteria accordingly.
Permanent methods, such as tubal ligation and vasectomy should be discouraged for adolescents and youth without children
Any adolescent and youth who requests emergency contraception should receive counseling on all methods of FP
Adolescents may be less tolerant of side effects. It is important to explain the possible side effects during FP counseling in order to reduce the likelihood of discontinuation and seek alternative methods if the side effects persist.
The National Family Planning Guidelines align with the 2015 World Health Organization medical eligibility criteria guidelines. Therefore, Kenya is placed in the green category for this indicator.
Although the availability of emergency contraception (EC) is not factored into the categorization of this indicator, note that under these guidelines adolescents and youth are eligible to receive EC.
The cabinet secretaries of the Ministries of Education and Health have jointly signed the
National School Health Policy, 2019.
The Policy does not detail a standalone comprehensive sexuality education (CSE) program but rather integrates several of the United Nations Population Fund
s (UNFPA
s) essential components throughout the document, including the recognition of international and national equal rights to health reproductive health; an integrated focus on gender; access and links to sexual and reproductive health (SRH) information and services; a safe and healthy learning environment; and cultural relevance. However, the Policy does not clearly address the remaining four essential CSE elements: scientifically accurate information, participatory teaching methods, youth advocacy and civic engagement, and connections to the informal sector.
References to sexuality education are vague in the Policy. The most relevant section,
Early/Unprotected sexual activity
alludes to protectionist educational opportunities, such as abstinence, to learn about avoiding sexual situations but does not explicitly mention enabling educational practices, such as linking youth to SRH services or informing youth about contraception:
The design and production of educational materials shall be done in collaboration with Ministry of Education
KIE [Kenya Institute of Education] and Ministry of Public Health and Sanitation (MOPHS).
The adolescent reproductive health materials developed through MOPHS shall be reviewed for relevance in the various school classes
grades.
Schools shall equip students with adequate skills to avoid situations that would lead to teenage pregnancy, rape and sodomy.
All children, including those with special needs and disability, shall be protected from sexual violence and abuse.
Students shall be taught and instilled with skills to avoid health risks, including rape.
Students shall be taught about the consequences of involving themselves in sexual activities as these may lead to pregnancy, disease, infertility etc.
The
National Adolescent Sexual and Reproductive Health Policy, 2015,
includes more direct CSE guidance for educating youth. In the policy, CSE is defined as:
Age-Appropriate Comprehensive Sexuality Education is an age-appropriate, culturally relevant approach to teaching about sexuality and relationships by providing scientifically accurate, realistic and non-judgmental information. Sexuality education provides opportunities to explore one
s own values and attitudes as well as build decision-making communication and risk reduction skills about many aspects of sexuality.
The guidelines in the
National Adolescent Sexual and Reproductive Health Policy
and the
National Adolescent Sexual Reproductive Health Policy Implementation Framework, 2017-2021
lay out a vision for sexuality education in the country, including elements such as reaching in-school and out-of-school youth, using medically accurate information, and training health care providers to provide SRH information. Further, the
National Guidelines for Provision of Adolescent and Youth Friendly Services in Kenya, 2016
present a framework for youth-friendly service delivery based at schools. Included in this framework are components such as life skills education on decision-making, negotiation, self-assurance, and communication, as well as an emphasis on school discussions on the topic of sexual assault. None of these guidelines, however, cover all nine essential components of CSE.
The policy environment surrounding CSE in Kenya is considered promising but incomplete, and the country has been placed in the yellow category for this indicator.
Kenya has an inclusive and supportive policy environment for the provision of sexual and reproductive health (SRH) services to both youth and adolescents, incorporating the three service-delivery elements of youth-friendly contraceptive services . The
National Guidelines for Provision of Adolescent and Youth Friendly Services in Kenya, 2016
recognize the health and human rights of young people. The guidelines explicitly address the high cost of services as a barrier to youth seeking FP services:
All adolescents and youth should be able to receive health services free of charge or are able to afford any charges that might be in place.
The National Guidelines recognize and address the challenges providers face when balancing personal beliefs with the provision of SRH care to youth:
Health service providers report being torn between personal feelings, cultural and religious values and beliefs and their wish to respect young people
s rights to accessing and obtaining SRH services. Training of service providers should address service provider attitudes and beliefs, and improve provider knowledge of normal adolescent development and special characteristics of adolescent clients and skills
both clinical and counselling.
The
National Family Planning Guidelines for Service Providers, 2016
further reference offering nonjudgmental and private contraceptive services:
Health service providers should receive both pre- and in-service training on but not limited to:
- Essential package for AYFS [adolescent and youth-friendly services]
- Value clarification and attitude transformation
- (VCAT) training on adolescent and
youth sexuality and provision of services such as
contraception
- Characteristics of adolescent growth and development (including neurobiological,
developmental and physical) which impact health
- Privacy and confidentiality
The
National Adolescent Sexual Reproductive Health Policy Implementation Framework, 2017-2021
also outlines several planned activities to expand and improve provider training on adolescent and youth-friendly services.
Since the policy environment addresses the three core elements of youth-friendly service provision, Kenya is placed in the green category for this indicator.
Thematic Area 5 of Kenya
National Family Planning Costed Implementation Plan, 2017-2020
outlines several activities to promote FP within the community, one of which targets support for adolescent sexual and reproductive health:
Activity DC 2. Adaptation of a multisectoral/stakeholder approach in provision of accurate and consistent information on FP to communities.
DC 2.1.3. FP coordinators to support adolescents and youth to promote FP among peers.
The
National Adolescent Sexual and Reproductive Health Policy, 2015
states an objective to
promote adolescent sexual and reproductive health and rights
and includes specific actions relevant to building community support and addressing gender norms:
Promote education of parents and the community on Sexual and Reproductive Health and Rights of adolescents
Mainstream gender and address its concerns in all ASRH [adolescent sexual and reproductive health] programs.
Both actions are further detailed in
The
National Adolescent Sexual Reproductive Health Policy Implementation Framework, 2017-2021.
Additionally, the
National Guidelines for Provision of Adolescent and Youth Friendly Services in Kenya, 2016
recognize the compounding impact of gender norms for youth accessing FP:
Gender inequities and differences that characterize the social, cultural and economic lives of the young people influence their health and development. Thus, adolescents and youth friendly reproductive and sexual health services must promote gender equality
All three policies seek to create an enabling social environment for youth FP, placing Kenya in the green category for this indicator.
The
Loi no2017-043 fixant les r
gles g
rales r
gissant la sant
de la reproduction et la planification familiale
addresses an individual
s right to plan their family without consent from their partner:
Article 4.-Toute personne a le droit de fonder une famille, de procr
er ainsi que de
D
cider librement avec discernement du nombre d
enfants de l
espacement des naissances et ce, ind
pendamment de l
autorisation de son partenaire.
The
Manuel de r
rence pour la formation des prestataires de services en sant
des adolescents et jeunes, 2018
outlines the roles and qualities that reproductive health providers should adopt when treating adolescents and young people, including ensuring access to services without requiring parental consent:
3.3 R
les et qualit
un bon prestataire
Tableau 6
: Qualit
un bon prestataire
Un prestataire de service de sant
qui interagit avec les adolescents et les jeunes devrait poss
der, pratiquer et ma
triser les caract
ristiques d
une communication efficace suivantes
- Assurer la confidentialit
: conseiller et traiter les adolescents et les jeunes avec ou sans le consentement des parents et des tuteurs, mais privil
gier le consentement volontaire inform
;
These adolescent and health services include contraceptive methods:
4.4 Avantages de la contraception pour les adolescentes
- Report de l
ge de la premi
re grossesse
;
- Pr
vention des grossesses pr
coces et non d
;
- Pr
vention des infections sexuellement transmissible y compris le VIH/SIDA
;
- Faible d
perdition scolaire.
4.5 M
thodes de contraception pour les adolescents et jeunes
Les prestataires de service de sant
doivent avoir
:
- avoir d
une mani
re g
rale des comp
tences particuli
res en mati
re de contraception et plus particuli
rement chez les adolescents.
- ma
triser les m
thodes contraceptives adapt
es aux adolescents.
Madagascar is placed in the yellow category for this indicator because its policies support youth access to FP services without consent from parents but does not address consent from spouses.
The "Loi n
2017-043 fixant les r
gles g
rales r
gissant la sant
de la reproduction et la planification familiale" states that providers are obligated to respect a patient
s confidentiality and individual choice in family planning
:
Article 14- Article 14.- L'obligation de confidentialit
de respecter les r
gles de d
ontologie, d'informer de respecter le choix des individus est impos
e aux prestataires de soins de la
Sant
de la Reproduction et de la Planification Familiale.
The
Normes et proc
dures en sant
de la reproduction, 2017
state that all clients have the right to access services without discrimination and that providers must adhere to the terms of counseling, provide impartial and complete information, and put aside personal prejudices when providing reproductive health services:
Droit
s aux services
- S
assurer que les services atteindront, sans discrimination, tous les individus qui en ont besoin, m
me ceux pour qui les services r
guliers de sant
ne sont pas facilement accessibles notamment pour les adolescents et jeunes.
Droit
la libert
de choix
-Fournir des informations impartiales et compl
tes, pour permettre un choix libre et
clair
par le/la patient(e)
: choisir le lieu, le type de prestataire, la modalit
obtention des soins
-Assurer la disponibilit
une gamme compl
te en intrants SR [sant
reproductive].
Droit
la dignit
Traiter les patients avec courtoisie, consid
ration, attention, et avec le total respect de leur dignit
, sans consid
ration de leur niveau d
instruction, statut social, ou tout autre caract
ristique qui peut les singulariser ou les faire d
nigrer.
Mettre de c
ses pr
s personnels, de genre, d
tat civil, de statut social ainsi que ses pr
s et attitudes intellectuelles.
The
Normes
also require service providers to use the medical eligibility criteria when providing contraceptives and notes that providers should respect the terms of counseling to youth:
2.
Offre de service PF aux adolescents et aux jeunes
Premier contact
: CSB
[centre de sant
de base] (Sages-femmes, infirmiers et m
decins g
ralistes)
- Bien accueillir les adolescents et les jeunes, avec intimit
, confidentialit
et convivialit
- Conseiller les adolescents et jeunes qui demandent de l
aide tout en respectant les modalit
s en counseling
- Informer les jeunes (sexuellement actifs ou non sur le planning familial
- Donner la possibilit
un choix
clair
sur la Planification Familiale [PF]
- Offrir un service de PF en expliquant l
importance, les avantages et effets ind
sirables, avec les moyens de les g
rer
While the law underscores the providers
obligation to respect youth choice in reproductive health and family planning and directs them to use medical eligibility criteria, it does not address nonmedical provider authorization. Madagascar is therefore placed in the yellow category for this indicator.
The "Loi n
2017-043 fixant les r
gles g
rales r
gissant la sant
de la reproduction et la planification familiale" states that all individuals have the right to reproductive health and family planning regardless of age or marital status:
Article 3.
Tous les individus sont
gaux en droit et en dignit
en mati
re de sant
de la reproduction. Chaque individu sans discrimination, peut mener une vie sexuelle responsable et sans risque.
Le droit
la Sant
de la Reproduction et
la Planification Familiale est un droit fondamental.
Aucun individu ne peut
tre priv
de ce droit dont il b
ficie sans discrimination
Aucune fond
e sur l'
ge, le sexe, la fortune, la couleur, de la peau, la religion, l'ethnie, la situation matrimoniale ou sur toute autre situation.
Madagascar is placed in the green category for this indicator as the law supports youth access to FP services regardless of age.
The "Loi n
2017-043 fixant les r
gles g
rales r
gissant la sant
de la reproduction et la planification familiale" states that all individuals have the right to reproductive health and family planning regardless of age or marital status:
Article 3.
Tous les individus sont
gaux en droit et en dignit
en mati
re de sant
de la reproduction. Chaque individu sans discrimination, peut mener une vie sexuelle responsable et sans risque.
Le droit
la Sant
de la Reproduction et
la Planification Familiale est un droit fondamental.
Aucun individu ne peut
tre priv
de ce droit dont il b
ficie sans discrimination aucune fond
e sur l'
ge, le sexe, la fortune, la couleur, de la peau, la religion, l'ethnie, la situation matrimoniale ou sur toute autre situation.
The law also states that young people and adolescents can access reproductive healthcare regardless of marital status:
Article 21: Les soins et prestations de services de Sant
de la Reproduction comprenant, entre autres, les composantes suivantes
3) la sant
reproductive des jeunes et adolescents
: Conseils et offre de service de Planification Familiale pour les adolescents sexuellement actifs mari
s ou non;
Madagascar is placed in the green category for this indicator because the policy environment confirms that youth must be permitted access to FP services regardless of marital status.
The "Loi n
2017-043 fixant les r
gles g
rales r
gissant la sant
de la reproduction et la planification familiale" supports an individual
s right to information on a range of contraceptive methods:
Article 3
Chaque individu a droit
information, a l
ducation concernant les avantages, les risques et l
efficacit
de toutes les m
thodes contraceptives.
The "Plan d
action national budg
en planification familiale
Madagascar, 2016-2020" includes a strategic priority on adolescent contraceptive demand creation through information on modern methods:
Priorit
2 : Cr
er la demande aupr
s de la population, surtout les jeunes,
travers des informations correctes et appropri
es sur les m
thodes modernes de PF et des points de services.
The
Plan d
action
also outlines a strategy to increase the range of methods available to young people, including long-acting reversible contraceptives (LARCs):
Des strat
gies vont
tre mises en place pour rem
dier aux probl
mes de manque de formation du personnel, renforcer les comp
tences des prestataires en PF, am
liorer l
offre de la gamme des produits contraceptifs de qualit
, notamment des m
thodes modernes et de longue dur
e et enfin favoriser l
la PF de qualit
pour tous, surtout parmi les jeunes.
The "Plan de d
veloppement du secteur sant
, 2020-2024" includes an objective to expand the range of contraceptives available in Madagascar without specifying youth and adolescents as beneficiaries:
Produit
1.1.6: Le contr
le de naissance et la lutte contre la grossesse non d
e est am
lior
e
Grandes lignes d
interventions
- Vulgarisation et valorisation des NTIC dans l
ducation sur les m
thodes contraceptives naturelles
et modernes
- Extension des offres de service PF au niveau communautaire
- Implication effective des hommes dans la PF
- Extension de la gamme de produits contraceptifs
Madagascar's policies outline strategies for increasing youth access to a range of methods, including LARCs. Therefore, Madagascar is placed in the green category for this indicator.
Although the availability of emergency contraception (EC) is not factored into the categorization of this indicator, note that the
Plan d
action
includes EC in its plans to promote and scale up long-acting and new contraceptive methods, but not in the adolescent-specific section on sexual and reproductive health. Thus, it is unclear whether the policy intends for EC to be accessible to youth.
The "Loi n
2017-043 fixant les r
gles g
rales r
gissant la sant
de la reproduction et la planification familiale" aims to ensure universal access to FP education:
Objectif 3.7 : Assurer l'acc
s de tous
des services de soins de sant
sexuelle et procr
ative, y compris des fins de la planification familiale, d 'information et d'
ducation, et la prise en compte de la sant
procr
ative dans les strat
gies et programmes nationaux
The
Plan d
action national budg
en planification familiale
Madagascar, 2016-2020
also states the need for reproductive health advocacy and describes an activity to advocate for sexual health education:
CD 2.5 Mettre l
accent sur la sensibilisation des jeunes par rapport
la PF et aux dangers li
la grossesse pr
coce. Les jeunes repr
sentent une population vuln
rable avec des besoins souvent insatisfaits en raison des barri
res culturelles et institutionnelles. Le premier lieu d
ducation des jeunes est l
cole. Ainsi, le plaidoyer sera fait
travers la vulgarisation de l
ducation sexuelle dans les
coles publiques et priv
es vers les professeurs form
s.
The
Plan strat
gique national en sant
de la reproduction des adolescents et des jeunes, 2018-2020
outlines a strategic focus to strengthen access to information that meets adolescents
and young people
s needs, including interventions in schools:
Axe strat
gique 2 : Renforcement de l
s aux informations r
pondant aux besoins des adolescents et des jeunes ainsi que des personnes influentes par une communication strat
gique
Interventions Prioritaires
5.4 Int
grer la SRAJ [sant
reproductive des adolescents et des jeunes]
dans le paquet d
activit
s des
tablissements scolaires, des centres sociaux, des Centres d
information et de prise en charge du PVVIH [personne vivant avec le virus de l
immunod
ficience humaine]
5.5 Int
grer le programme d
ducation par le pair dans les associations caritatives, confessionnelles et du scoutisme (Kiady, Fanilo, Mpanazava, Tily, Antily...)...
5.7 Poursuivre l
gration de la SRAJ dans les
coles, centres de formation militaires, garnisons et centres de r
ducation p
nitentiaires
The "Plan strategique" also lists integration of a comprehensive sexuality education (CSE) program into the public and private school curriculum as a key output:
Produit 7
: Des programmes d
information, d
ducation et d
orientation en mati
re de SSRAJ ciblant les adolescents et les jeunes sont disponibles et int
es dans le programme scolaire public et priv
.
7 .1 - Mettre
chelle le programme d
Education Sexuelle Compl
te au sein des
tablissements d
enseignement primaire, secondaire publiques et priv
s
The
Plan strategique
also lists activities to broaden the reach of a CSE program to out-of-school youth:
6.3 Adapter le programme d
ducation sexuelle compl
te pour les jeunes non scolaris
s 6.4 Adapter les modules sur la SRAJ dans les programmes d
alphab
tisation pour la formation de jeunes d
scolaris
s et non scolaris
s, et les centres pour les personnes en situation d
handicap
Finally, the "Plan sectoriel de l'
ducation, 2018-2022" outlines the priorities for school health, including the acquisition of responsible health behaviors:
Promouvoir la sant
des Jeunes :
En mati
re de la sant
des jeunes, il y a lieu d
augmenter l
accessibilit
des jeunes scolaris
s aux informations en mati
re de Sant
des Jeunes
travers des actions de sensibilisation au niveau des coll
ges et lyc
es afin de leur faire acqu
rir des comportements responsables en mati
re de Sant
des Jeunes et Adolescents.
The Plan sectoriel" identifies an activity for the next draft of the Malagasy curriculum as the introduction of education on adolescent reproductive health:
Les activit
mettre en
uvre pour
laborer le deuxi
me draft du u Cadre d
orientation et d
organisation du curriculum malagasy sont :
- la r
flexion sur l
introduction des TICE [technologie de l'information et de la communication en
ducation], les comp
tences pour la vie dont l
ducation sexuelle qui englobe la sant
reproductive des adolescents (SRA ) et l
ducation des filles, la sant
scolaire, l
ducation inclusive, l
ducation
la citoyennet
ducation
la paix, la lutte contre la corruption, l
EDD [
ducation au d
veloppement durable] avec int
gration des th
mes
ducation civique,
ducation environnementale,
ducation maritime.
The
Strategie nationale de lutte contre le mariage des enfants, 2017-2024
discusses several approaches to increase sexual and reproductive health knowledge among adolescents and young people, including in and out of schools:
Axe Strat
gique 2.1
Promouvoir la sant
et le bien-
tre pour assurer la r
duction de la vuln
rabilit
des jeunes visant le changement de leur comportement li
la sexualit
211-Renforcer et intensifier la diffusion des informations et la communication interpersonnelle sur la sant
reproductive, la sexualit
et les services disponibles aupr
s des enfants et jeunes
212- Renforcer/Inclure dans le Programme scolaire l'
ducation sur la sant
sexuelle et de reproduction
213-Conseiller et accompagner les adolescents dans leur choix de comportement sexuel pour s
auto-prot
ger contre le mariage et la grossesse pr
coces
214-Renforcer l'
ducation sur la sant
sexuelle et de reproduction pour les enfants en dehors du syst
me scolaire.
In its strategy to raise awareness of reproductive health and FP among adolescents and youth, the
Plan strat
gique int
en planification familiale et en
curisation des produits de sant
de la reproduction, 2021-2025
specifically addresses scaling up CSE based on the United Nations Educational, Scientific and Cultural Organization (UNESCO) guiding principles:
Objectif sp
cifique 1.1
duire de 28,9 %
25% la proportion des adolescentes (15-19 ans) ayant d
eu un enfant
Tableau 3 : Orientation strat
giques et axes prioritaires
Strat
gies
: Renforcement des actions de sensibilisations en SR/PF adapt
chaque tranche d
ge pour les adolescents et les jeunes
Actions prioritaires
- Mise
chelle de l
ducation compl
la sexualit
bas
e sur les principes directeurs de l
UNESCO
The sexual and reproductive education strategies discussed in the
Plan strat
gique
include strengthening FP communication strategies for in and out-of-school youth:
Strategies
:
- Renforcement des strat
gies de communication en direction des jeunes scolaris
s et non scolaris
s.
R
sultats
attendus
- Les jeunes et les adolescents fr
quentant les CSB amis des jeunes, les r
seaux de services
Amis des jeunes
sont conscients des avantages de la SR/PF et des dangers li
la grossesse pr
coce et en adoptent des comportements sains
- Les
ves des
coles publiques et priv
es des Chefs-lieux des 113 Districts Sanitaires sont inform
s et sensibilis
s sur l
ducation
la sexualit
et adoptent des comportements sains en mati
re de SR et de PF
- Les jeunes sont sensibilis
s sur les avantages de la PF, sur les dangers li
la grossesse et l
accouchement et adoptent des comportements sains gr
ce aux TIC (SMS, internet).
Madagascar
s policy environment is supportive of sexuality education but does not outline a detailed CSE policy referencing all nine of the United Nations Population Fund (UNFPA) essential components. Therefore, Madagascar is placed in the yellow category for this indicator.
The "Loi n
2017-043 fixant les r
gles g
rales r
gissant la sant
de la reproduction et la planification familiale" states that providers are obligated to respect a patient
s confidentiality and individual choice in family planning:
Article 14- Article 14.- L'obligation de confidentialit
de respecter les r
gles de d
ontologie, d'informer de respecter le choix des individus est impos
e aux prestataires de soins de la Sant
de la Reproduction et de la Planification Familiale.
The "Plan strat
gique national en sant
de la reproduction des adolescents et des jeunes, 2018-2020" outlines activities to reinforce the competencies of service providers, including training service providers on youth-
friendly services:
Axe strat
gique 3 : Renforcement de capacit
s institutionnelles et des comp
tences techniques et manag
riales des acteurs impliqu
s dans la mise en
uvre du PSN [plan strat
gique national], y compris les adolescents et les jeunes.
Interventions
:
8.1 Instaurer un service convivial de SRAJ [sant
reproductive des adolescents et des jeunes] avec renforcement en sensibilisations bas
es sur la pr
vention dans la structure de prise en charge des cas de situation d
urgence ;
8.2. Former les prestataires de services (m
decin, sage-femme, assistants sociaux ; responsable des centres sociaux, AC [agent communautaire], centre de r
ducation et de r
insertion sociale, intervenants sociaux) sur les techniques de communication au profit des groupes sp
cifiques des adolescents et des jeunes ;
8.3. D
velopper et mettre en
uvre des strat
gies avanc
es pour les jeunes de rue, les jeunes d
linquants, les jeunes de la population cl
haut risque, les jeunes en situation d
handicap, les jeunes en couple et les jeunes parents ;
8.4. D
velopper et mettre
chelle les offres communautaires pour les jeunes en union et jeune parent pour la premi
re fois en utilisant les services de sant
disponibles et les
nements
communautaires ;
The "Plan strat
gique " also details the recipients of training activities on adolescent health, including providers, managerial staff, and referral staff:
Axe Strat
gique 4
: Offre de services de sant
communautaires et cliniques int
s de SSRAJ de qualit
et conviviaux adapt
s aux adolescents et jeunes
Interventions
:
12.1 Identifier les besoins de formation et de renforcement de capacit
s techniques des prestataires et des superviseurs
tous les diff
rents niveaux en mati
re de SRAJ
12.2
laborer
le kit de formation de capacit
s techniques et manag
riales
intention des prestataires et des superviseurs
12.3 D
velopper le syst
me de r
rence et de contre r
rence
partir du niveau communautaire
12.4 Assurer la formation de prestataires de services sur les techniques d
offre de services SSRAJ [sant
sexuelle et reproductive des adolescents et des jeunes] aux adolescents et jeunes
12.5. Former le personnel d
appui en accueil et orientation des adolescents et des jeunes clients 12.6 Assurer la formation manag
riale et les visites d
changes d
riences pour les gestionnaires de programmes
divers niveaux (secteurs public et priv
) sur les dispositifs d
offre de service de SSRAJ
The "Plan d
action national budg
en planification familiale
Madagascar, 2016-2020" describes additional activities to train service providers to better provide services to young people, including training to reduce bias, stigma, and discrimination:
OAS 3.7 Renforcement de l
approche jeune dans la prestation de services PF.
De nouveaux espaces jeunes, de nouveaux centres amis des jeunes, coins et kiosques des jeunes vont
galement
tre cr
s dans plus de 25% des CSB [centres de sant
de base] publics de chaque district sanitaire qui vont
tre transform
s en CSB
Ami des Jeunes
. Ils seront, en outre, mis aux normes en mati
re d
IEC [information,
ducation et communication]/CCC [communication pour le changement de comportement]. Enfin, le personnel de sant
va
tre form
IEC/CCC en PF et
approche jeune permettant ainsi une meilleure prise en charge de cette tranche de la population.
OAS 3.7.3 Transformer des CSB2 des 113 DS en CSB Amis des jeunes Paravent pour confidentialit
OAS 3.7.3.1 Identifier des CSB
transformer en CSB Amis des jeunes (salle pour accueil des jeunes, personnel de sant
suffisant, ...)
OAS 3.7.3.3 Former des formateurs en SRA [sant
de la reproduction des adolescents]/approche jeune
The
Normes et proc
dures en sant
de la reproduction, 2017
also outline the family planning services available to adolescents and youth at varying levels of the health system. All levels emphasize ensuring privacy and confidentiality, providing accurate FP information on all methods, and ensuring free method choice in FP services and counseling.
The
Politique nationale de sant
des adolescents et des jeunes, 2019
also lays out the required conditions for adolescents and youth-friendly service provision, and emphasizes the affordability of services and nondiscrimination toward adolescents and young people:
2. Acc
s facile aux services des adolescents et des jeunes.
La politique pr
voit l
lioration de l
s aux services
travers :
-la disponibilit
de l
offre de services de qualit
en sant
des adolescents et des jeunes, adapt
leurs besoins : accessibles, acceptables, abordables,
quitables, ad
quats, efficaces et p
rennes ;
-l
augmentation de l
utilisation des services sera renforc
e par le biais de la stimulation de la demande ;
la disponibilit
et la diffusion des informations sur les offres de service en sant
des adolescents et des jeunes ;
-l
application des lois en vigueur concernant les droits en sant
sexuelle et reproductive des adolescents et des jeunes ;
-la non-discrimination et la non stigmatisation envers les adolescents et les jeunes.
The "Plan d
action" references a Malagasy policy signed in 2006 that includes a provision of free FP products and services, but the policy could not be located for review. As reviewed policies address training and supporting providers and enforcing confidentiality but do not sufficiently address the cost of services, Madagascar is placed in the yellow category for this indicator.
The "Loi n
2017-043 fixant les r
gles g
rales r
gissant la sant
de la reproduction et la planification familiale" outlines the importance of male involvement in reproductive health (RH):
Article 16 : Les personnes du genre masculin ont le devoir de prot
ger le droit des femmes
la sant
sexuelle et reproductive de ces derni
res, notamment leur acc
s aux services et le respect de leur choix sur la procr
ation.
The "Plan strat
gique national en sant
de la reproduction des adolescents et des jeunes, 2018-2020" outlines community dialogues as a priority intervention:
Interventions Prioritaires
:
1.3 Programmer des dialogues communautaires pour discuter des droits des jeunes et des comportements responsables en leur faveur
The "Plan strat
gique" provides further clarity in detailed strategic communication activities to enable support for youth access to RH services:
Interventions Prioritaires :...
5.9 Renforcer les capacit
s des acteurs/communaut
ducative (parents et animateurs, AC [agent communautaire],
ducateurs, jeunes leaders, agents de sant
) sur la SRAJ [sant
reproductive des adolescents et des jeunes], communication pour le changement social et comportemental des jeunes, et l
orientation vers les services
Axe strat
gique 2 : Renforcement de l
s aux informations r
pondant aux besoins des adolescents et des jeunes ainsi que des personnes influentes par une communication strat
gique...
6.2 Recenser et orienter les activit
s de communication/ sensibilisation sur SRAJ dans les centres d
coute, centres de promotion sociale, centres de jeunesse et au niveau des organisations de sports et des loisirs avec un accent sur le genre et le r
rencement...
6.9 Organiser des s
ances de communication au profit des personnes influentes, des adolescents et des jeunes en vue de leur appui dans l
orientation des jeunes (parents) vers les services SSRAJ
[sant
sexuelle et reproductive des adolescents et des jeunes]
The
Plan strat
gique
includes other activities to target traditional and religious leaders and others influential in the community to build their capacity to defend adolescent and youth reproductive health:
9.1 Renforcer et mettre
chelle un programme d
ducation des parents au niveau communautaire et autour des structures d
encadrement des adolescents et jeunes
9.2 Renforcer les comp
tences des APART [autorit
s politiques administratives religieuses et traditionnelles] en vue de mieux d
fendre les int
ts des groupes d
adolescents et jeunes vuln
rables en mati
re de SSRAJ
9.3 Elaborer et diffuser un catalogue/ r
pertoire renfermant tous les supports IEC [information-
ducation-communication] disponibles pour faciliter l
s aux utilisateurs
9.4 Organiser des dialogues communautaires et d
bats m
diatiques et
nementielles
impliquant les autorit
s et les leaders traditionnels (APART) sur la question SSRAJ notamment sur le mariage des enfants et la grossesse pr
coce
9.5 Organiser des dialogues communautaires entre parents et adolescents portant sur les obstacles culturels
la promotion de la SSRAJ
9.6 Appuyer les CTD [collectivit
s locales d
centralis
es] et les organisations confessionnelles pour l
gration des activit
s SSRAJ dans leurs priorit
actions
The "Plan sectoriel de l
ducation, 2018-2022" includes activities to build support within the community for adolescent RH awareness and acknowledges the challenges that young girls face:
En se r
rant
la partie
Education Inclusive
du pr
sent Plan Sectoriel de l
Education, la discrimination en termes de genre handicape les jeunes filles et a un impact s
rieux sur leur scolarisation. Les parents ont assur
ment une place importante
assurer aupr
s des jeunes et notamment des jeunes filles dans leur
ducation
la notion de genre et
la sant
reproductive. Cependant, parler de ces sujets et notamment de la sant
reproductive reste tabou dans certaines familles malgaches, et plus particuli
rement dans les zones d
favoris
es.
The "Plan sectoriel" includes activities to strengthen parents
knowledge of youth sexual and reproductive health through an awareness campaign in collaboration with local radio stations, as well as educating parents and the community on the importance and necessity of sexual health education.
The
Plan d
action national budg
en planification familiale
Madagascar, 2016-2020" also lays out a detailed strategy to strengthen the environment for family planning through community engagement and mobilization. The proposed activities include an information campaign to bridge religious and cultural gaps toward acceptance and use of family planning but fail to specifically address youth access. The
Plan d
action
emphasizes the importance of involving men and husbands in family planning, and proposes an information campaign to specifically address the specific needs of young people:
Des efforts particuliers pour la cr
ation de la demande vont
tre faits pour les hommes et les jeunes. Les hommes partagent autant de responsabilit
s que les femmes dans la sant
de la reproduction. N
anmoins, le manque d
attention leur
tant port
e sugg
re que la PF ne les concerne pas. L
implication des hommes et des maris est cruciale pour le succ
s des campagnes de cr
ation de la demande. Les hommes peuvent emp
cher les femmes d
utiliser la PF et ainsi d
y avoir recours librement. C
est en r
duisant leurs pr
s que l
on assurera leur soutien pour la PF. Pour r
pondre aux besoins sp
cifiques des jeunes, des campagnes d
information sp
cifiques vont
tre mises en place. Elles insisteront sur les dangers des grossesses pr
coces et sur les bienfaits de la contraception
Additional policy documents also outline strategies for increasing community support for youth FP, including the
Normes et proc
dures en sant
de la reproduction, 2017,
which works to sensitize community leaders in favor of adolescent RH services, and the
Plan strat
gique int
en planification familiale et en
curisation des produits de sant
de la reproduction, 2021-2025,
which includes a strategy to involve social and religious leaders in community dialogues to gain their support for the new reproductive health law, which supports youth FP.
The
Plan strat
gique int
en planification familiale
also targets male reluctance around contraceptive use in its awareness and advocacy campaigns:
Strat
gies
Renforcement des campagnes d
information, de sensibilisation et de plaidoyer sur la SR [sant
reproductive]/PF aupr
s de la population
Actions prioritaires
- Promotion de la masculinit
positive (groupes d'hommes, groupes de papas) en vue de sensibiliser ceux et celles qui sont r
ticents
utilisation des m
thodes contraceptives modernes
Madagascar
s policies outline specific interventions to build support within the larger community for youth FP and address gender and social norms. Madagascar is therefore placed in the green category for this indicator.
The
Malawi Costed Implementation Plan for Family Planning, 2016-2020
notes that the country
s family planning approach includes access to services without third-party authorization:
Malawi employs a rights-based approach to family planning that includes voluntarism, informed choice, free and informed consent, respect to privacy and confidentiality without having to seek third party authorization, equality and non-discrimination, equity, quality, client-centered care, and participation and accountability.
The
Preservice Education Family Planning Reference Guide, 2010
confirms adolescents
right to access contraceptives without third-party authorization:
Adolescents need to know:
- That [contraceptive] methods are available to them and that they are not required to have parental or spousal consent to receive a contraceptive method.
Malawi is placed in the green category for this indicator as its policies support youth access to family planning services without consent from parents and spouses.
The
Preservice Education Family Planning Reference Guide, 2010
provides information and training activities on family planning for health care providers. The
Family Planning Counseling
section emphasizes clients
informed choice and their rights to accurate FP information and access to services without discrimination. It further details the characteristics a provider should adopt providing services:
Quality counselling is the main way that health workers support and safeguard the client
s rights to informed and voluntary decision-making. (See Section 6.3.) This means never pressuring a client to choose one family planning method over another, or otherwise limiting a client
s choices for any reason other than medical eligibility. Counselling can support all other clients
rights as well (ACQUIRE Project 2008).
The key principles for cultivating good client-provider interaction and effective family planning counseling include the following:
- Remain nonjudgmental about values, behaviours, and decisions that differ from your own.
The Reference Guide also includes World Health Organization medical eligibility criteria (MEC)
which is grounded in medical authorization and can be used to reduce unjustified barriers to FP services
by evidence
also includes a two-category medical eligibility criteria system for use where resources for clinical judgment are limited. The Reference Guide notes that the MEC are not intended as a national guideline for family planning but rather as a reference. The Reference Guide does, however, continue to reinforce adolescents
medical eligibility for contraception:
21.9 Adolescent Contraception
Adolescents are medically eligible to use any method of contraception and must have access to a variety of contraceptive choices.
Moreover, the
Malawi National Reproductive Health Service Delivery Guidelines, 2014-2019," require health workers to ensure a
friendly, non-judgmental, and welcome
approach in providing adolescent/youth sexual and reproductive health services, including family planning services.
While Malawi
s policies acknowledge the barriers that provider bias and judgment place on access to family planning and note that providers must use clinical judgment when providing contraceptives, the policy language does not explicitly require providers to service youth despite personal beliefs. Malawi is placed in the yellow category for this indicator.
The
National Health Policy, 2017
notes that health administration in Malawi employs a human rights-based approach:
All the people of Malawi shall have the right to good health, and equitable access to health services without any form of discrimination, whether be it based on ethnicity, gender, age, disability, religion, political belief, geographical location, or economic and/or other social conditions.
The
National Sexual and Reproductive Health and Rights Policy, 2017-2022
reiterates the human-rights based approach when it comes to young people accessing sexual and reproductive health services:
3.6 Young people in Reproductive Health
3.6.2 Policy Statements
3.6.2.1 All young people shall have access to quality youth friendly health services that are safe, guard their right to privacy, ensure confidentiality, and provide respect and informed consent, while also respecting their cultural values and religious beliefs.
The
Preservice Education Family Planning Reference Guide, 2010
confirms that this approach also applies specifically to family planning by stating that youth should have access to any method of contraception regardless of age:
21.9 Adolescent Contraception
Adolescents are medically eligible to use any method of contraception and must have access to a variety of contraceptive choices. Age alone does not constitute a medical reason for denying any method to adolescents.
Malawi
s policies include policy affirmations of youth access to family planning regardless of age. Therefore, Malawi is placed in the green category for this indicator.
The
Preservice Education Family Planning Reference Guide, 2010
clearly states that youth should have access to family planning services regardless of marital status:
Right to access to services: Services must be affordable and available, without social barriers such as discrimination based on gender, age, marital status, fertility, nationality or ethnicity, belief, social class, caste, or sexual orientation.
The "Gender Equality Act, 2013" reinforces that access to FP should be provided regardless of marital status:
...every health officer shall:
(a) respect the sexual and reproductive health rights of every person without discrimination;
(c) provide family planning services to any person demanding the services irrespective of marital status or whether that person is accompanied by a spouse;
Because the law supports access to FP services regardless of marital status, Malawi is placed in the green category for this indicator.
The
National Sexual and Reproductive Health and Rights Policy, 2017-2022
acknowledges that public health facilities need to offer a full range of methods to reduce unmet need for young people:
3.1. 1 Family Planning Policy Goal
To reduce unmet need for family planning services through provision of voluntary comprehensive family planning services at all levels to all men, women and young people of reproductive age.
3.1.2 Policy Statements
3.1.2.2 Public health facilities shall offer a full range of family planning services, including emergency contraception.
3.1.2.7 Availability of long acting and permanent methods of contraceptives shall be expanded at all levels of health care service.
3.1.2.10 Emergency contraception shall be made available to all women who have had unprotected sex.
The
Preservice Education Family Planning Reference Guide, 2010
further details the medical eligibility criteria for adolescents, confirming safety and accessibility of all methods for adolescents:
21.8 Medical Eligibility Criteria for Adolescents
All contraceptive methods are safe for adolescents.
21.9 Adolescent Contraception
Adolescents are medically eligible to use any method of contraception and must have access to a variety of contraceptive choices. Age alone does not constitute a medical reason for denying any method to adolescents. While some concerns have been expressed regarding adolescents
use of certain contraceptive methods
(such as DMPA [depot medroxyprogesterone acetate] by youth under 18), these concerns must be balanced against the advantages of avoiding pregnancy. Social and behavioural issues should be important considerations in the choice of contraceptive methods by adolescents.
The Reference Guide provides additional considerations for specific methods, such as the privacy afforded by injectable use and dual protection against sexually transmitted infections by condoms, and clearly states that there is no medical reason to deny intrauterine devices or sterilization to young people. The Reference Guide also provides tables that summarize Malawi
s medical eligibility criteria for contraceptive use, which was summarized from the World Health Organization medical eligibility criteria policy, and acknowledges access to methods regardless of age, parity, and marital status.
As Malawi
s FP guidelines support youth access to a full range of FP methods regardless of age, marital status, and parity, Malawi is placed in the green category for this indictor.
While emergency contraception (EC) eligibility is not factored into this indicator
s rating, there is no clear age limit for young people to access EC even though the Reference Guide indicates no contraindications for EC pills for adolescent women.
Multiple Malawian policies advocate for the provision of sexuality education. The
National Plan of Action for Scaling Up SRH and HIV Prevention Initiatives for Young People, 2008-2012
includes objectives to increase life skills education for in-school youth:
Sub-objective 2.1.1. Scale Up Life Skills Education (LSE) for in-school young people.
Sub-objective 2.1.2 Scaled up LSE for out of school and vulnerable people.
Sub-objective 2.1.3: Scale up LSE for young people in work places.
Sub-objective 2.1.4: Improved and expanded SRH [sexual and reproductive health] peer education activities.
Sub-objective 2.1.5: Increase access to information on gender and legal literacy.
Sub-objective 2.1.6: Young women skilled in GBV [gender-based violence] prevention strategies.
Sub-objective 2.1.7: Increased access to alternative rites of passage program among young undergoing traditional initiation in selected communities.
Sub-objective 2.1.8: Increased exposure to BCC [behavior change communication] and edutainment activities using folk and mass media.
Sub-objective 2.1.9: Increased parent-child communication on SRH and HIV prevention issues in homes and communities.
The
National Youth Policy, 2013
advocates for the provision of comprehensive sexuality education (CSE) to increase youth uptake of family planning services:
3.6.3.2 Provision of comprehensive sexuality education that promotes abstinence, mutual faithfulness and condom use, uptake of family planning services amongst the youth is advocated.
The
Malawi Costed Implementation Plan for Family Planning, 2016-2020
mentions that the Ministry of Education, Science, and Technology has adopted a comprehensive
Life Skills and Sexual and Reproductive Health curriculum
for secondary school students, but a copy of the curriculum could not be reviewed for this analysis.
In the absence of a CSE curriculum that references all nine United Nations Population Fund (UNFPA) essential components, Malawi is placed in the yellow category for this indicator.
The
National Plan of Action for Scaling Up SRH and HIV Prevention Initiatives for Young People, 2008-2012
includes multiple activities to reach their strategic objective of increased utilization of quality youth-friendly sexual and reproductive health (SRH) services:
Sub-objective 3.1.1. YFHS [youth-friendly health services] SRH institutionalized into existing pre- and in-service training programs for health providers.
Sub-objective 3.1.2: Improved attitudes and competence of service delivery teams to provide quality YFHS.
Sub-objective 3.1.3 Improved facility environment and procedures.
Sub-objective 3.1.5: Improved access to quality YFHS by young people.
Sub-objective 3.1.6: increased availability of support services for young people.
Each sub-objective lays out certain key activities that can be taken to reach their desired input; relevant activities include training providers on attitude change and skills-building components for youth SRH and developing and equipping providers with appropriate job aids and tools to assist in delivery of quality services to youth.
The
Guidelines for Family Planning Communication, 2011
specifically note the barriers that youth face while seeking FP services, including negative attitudes of FP providers toward young people. The Guidelines further note that health workers impose barriers through provider bias when they
bring their own cultural and religious orientations to discussions about FP and make decisions on what is best for the client on that basis.
To address these barriers, the Guidelines note that youth have a right to access all health services, including FP services, and that providers should take the following actions:
Health workers
- Provide all clients, regardless of background, with comprehensive FP information and counseling so they can choose a suitable FP method.
- Encourage clients to return if they experience any unusual and persistent side effects with the method chosen.
- Help clients who are dissatisfied with their method to try a different method.
- Support women who have been sexually assaulted to access PEP [post-exposure prophylaxis] in a caring way. Help to refer them to other key legal and support services in a timely manner.
The
National Sexual and Reproductive Health and Rights Policy, 2017-2022
notes young people
s rights to SRH services that ensure privacy and confidentiality:
3.6.2 Young people in Reproductive Health Policy Statements
3.6.2.1 All young people shall have access to quality youth friendly health services that are safe, guard their right to privacy, ensure confidentiality, and provide respect and informed consent, while also respecting their cultural values and religious beliefs
The
Malawi Costed Implementation Plan for Family Planning, 2016-2020
acknowledges the biases that providers have against providing family planning for youth and note that in-service training should include rights-based services.
Strategic outcomes
SDA1. Health care workers are providing high-quality FP information and services and offering the full method mix to clients. In-service training will be reviewed to ensure training materials provide information on long-acting and reversible contraceptives (LARCs). Job aids will be updated, and supportive supervision will be conducted to ensure that health care providers are providing high-quality, rights-based information and services.
SDA6. Access to family planning by young people is safe, rights-based, and confidential. To increase the availability of YFHS, health workers, children
s corner patrons, and child representatives will be trained on these services. In addition, monitoring tools will be developed to track YFHS, and FP coordinators will be responsible for ensuring each facility in their district has staff providing the services.
The
Preservice Education Family Planning Reference Guide, 2010
notes that family planning providers should use multiple strategies to improve adolescents
access to FP services. The strategies include training providers to withhold judgment, providing confidentiality and ensuring audio/visual privacy, and offering services free or at low cost:
21.6 Improving Adolescents
Access to Family Planning Services
Improving adolescents
access to family planning services involves coordinated efforts by family planning providers, family planning service managers, and local and national health officials.
Strategies include:
- Training providers to offer
youth-friendly
counselling (see Section 21.7)
- Dedicating special areas of family planning clinics for adolescents, to help ensure privacy
- Using outreach and mobile clinics with staff trained to respond to adolescents
needs
- Offering clinic hours convenient for youth, such as after school and during weekends
- Locating services in convenient, safe areas
- Educating community-based contraceptive distributors and primary health workers (extension workers) about adolescents
challenges and needs and how they can assist them appropriately
- Offering youth a full range of family planning services, including ECPs [emergency contraception pills] and STI/HIV counselling and testing
- Providing psychosocial support and education about rape and harmful sexual practices and beliefs, such as ritual sexual cleansing
- Strengthening policies related to adolescent reproductive health services
- Obtaining political and community acceptance and support
- Offering services free or at low cost.
Malawi
National Youth Friendly Health Services Strategy, 2015-2020" includes a specific objective to enhance the capacity of service providers and implementing partners to deliver youth-friendly health services. To meet this objective, the Strategy identifies key activities that focus on the provision of on-the-job training, including the incorporation of youth-friendly health service standards among key competencies to be attained during pre-service trainings and the development of staff capacity in referral centers.
The policies reviewed clearly address the need to train and support providers to offer youth-friendly contraceptive services, as well as provide confidentiality and audio/visual privacy and free FP services. Malawi is placed in the green category for this indicator.
Malawi
National Population Policy, 2012
includes male involvement in reproductive health in its guiding principles and identifies two specific objectives that speak to creating an enabling environment for adolescent-friendly contraceptive services:
Recognizes the need to assist couples and individuals to fully meet their sexual and reproductive health rights and goals, with particular emphasis on male involvement in meeting women and their own reproductive health needs.
3.1.4 Policy Area 1: Specific Objective 3
To address cultural, religious, and other barriers of demand, access and use of family planning, including enhancing male involvement in reproductive health, enhancing the role of community members in
IEC [information, education, and communication] and distribution of contraceptives, and improving family planning commodity security.
3.1.5 Policy Area 1: Specific Objective 5
Enhance the role of national and local traditional, religious, and political leaders in championing population issues among Malawians.
Although not specific to youth access to family planning, the Population Policy recognizes the role that traditional leaders and community members can play in creating an environment supportive of family planning access and use:
Traditional Leaders and community members
The policy recognizes the important role that active participation of traditional leaders such as chiefs and communities at large play in implementation of development programmes at grassroots level. The policy will foster empowerment of traditional leaders to operate as champions of family planning; school enrolment, retention, and progression; reform or eradication of harmful traditional practices such as early marriage, and other population programmes. Community members will also enhance implementation of the policy through their active participation in planning, implementation, monitoring and evaluation. In particular, the policy will enhance the direct role of community members in enhancing IEC campaigns on the small-family norm and delivery of family planning and other reproductive health services within communities.
The
National Gender Policy, 2015
also includes four strategies to address gender within sexual and reproductive health:
Policy Priority Area 2: GENDER IN HEALTH
Objective 1: To improve women and girls
sexual and reproductive health rights
Strategy 1: Advocate for the modification and elimination of harmful cultural practices affecting reproductive health of women and girls and other vulnerable groups;
Strategy 2: Advocate for increased male involvement in reproductive health services;
Strategy 3: Promote awareness on the benefits of sexual and reproductive health services among women, men, girls and boys;
Strategy 4: Advocate for more user friendly health facilities and services that benefit women and girls, men and boys and vulnerable groups especially those in rural areas.
Within the strategic objective to create an enabling and supportive policy environment to improve SRH for young people, the
National Plan of Action for Scaling Up SRH and HIV Prevention Initiatives for Young People, 2008-2012
lays out multiple sub-objectives:
Faith and community leaders supportive of youth rights and enforcement of laws and policies
- Orient [youth action committees] and [youth technical committees] in advocacy and SRH and HIV/AIDS advocacy plan for young people
- Organize national religious leaders conference to review policies, programs and training curriculum of religious schools in relation to SRH, HIV prevention, some cultural practices and gender practices
- Target different cultural institutions with SRH/HIV interventions (Traditional leaders, traditional healers, Namkungwi
s, Angaliba and marriage counselors)
- Review cultural practices of each cultural group that have an impact on SRH and HIV and identify positive and negative practices (including which harmful practices to illuminate)
The National Plan of Action continues by addressing the need to build community support for youth SRH to reach increased utilization of quality youth-friendly SRH services:
Sub-objective 3.2.1 Increased support for YFHS [youth-friendly health services] among teachers, guardians, and the community leaders
Key Activity: Conduct participatory learning and action at the community level to engage parents, guardians, and community leaders on issues affecting young people in their communities, inform them about available YFHS services and solicit their support.
The
Guidelines for Family Planning Communication, 2011
specifically note the barriers that youth face while seeking FP services, including provider bias when they
bring their own cultural and religious orientations to discussions about FP and make decisions on what is best for the client on that basis
and discouragement from community leaders who do not support FP services for youth.
To address these barriers, the Guidelines outline accurate information that can be used in social and behavior change programming for various target groups, including community and religious leaders. The Guidelines continue to share multiple potential advocacy, social and community mobilization, and behavior change communication interventions that can be used to increase support for FP in the community.
The
Malawi Costed Implementation Plan for Family Planning, 2016-2020
also outlines strategies to engage community and traditional leaders as well as parents to increase support for FP:
DC3. Both partners are involved in FP decisions for their family and are supportive of the use of modern contraceptive by their partners. A key strategy to improve demand for family planning will be to engage chiefs and community leaders to provide accurate information about family planning to men in their communities. Traditional leaders will engage men through
husband school
to educate them on the benefits of family planning and address their questions and concerns. Additionally, the number of men who support the use of modern contraception for themselves or their partners will be increased by conducting community outreach events to engage men in FP dialogue and services.
DC5. Youth are supported to access FP information or services by their parents. Parents will be engaged through media, health workers, religious groups, and local outreach groups, such as mothers
groups and child support committees, to have discussions about sexual and reproductive health rights and issues with their children.
Malawi
s policies outline specific interventions to build support within the larger community for youth FP and address gender norms. Therefore, the country is placed in the green category for this indicator.
The "Loi n
02-044 relative
la sant
de la reproduction, 2002" states that spousal consent is required for permanent contraceptive methods except with a second medical opinion in the case of a life-threatening pregnancy:
Article 14 : Toute personne majeure peut, sur son consentement
crit, b
ficier d'une m
thode de contraception irr
versible. Toutefois, concernant une personne mari
e, l'accord de son conjoint est obligatoire. Sur avis m
dical confirm
par une contre-expertise, toute femme mari
e dont la vie pourrait
tre menac
e par la survivance d'une grossesse peut, sur son seul consentement
crit, b
ficier d'une m
thode de contraception irr
versible.
The
Politique et normes des services de sant
de la reproduction, 2019
reaffirms the law and clarifies that all contraceptives except permanent ones should be offered to all beneficiaries without parental or spousal consent:
3.4.1 La contraception
c. B
ficiaires
Les b
ficiaires des services de contraception sont les hommes, les femmes en
ge de procr
er et en particulier les femmes jeunes sans enfant, les grandes multipares, les personnes
comportement
risque des IST [infection sexuellement transmissible], VIH et Sida, les malades mentaux, les adolescents(es) et les jeunes, la famille et la communaut
. Les m
thodes de contraception,
exception des m
thodes permanentes (ligature des trompes et vasectomie) devront
tre offertes
tous les b
ficiaires qui en feront le choix, sans exiger l'autorisation ou le consentement parental ou marital.
The requirement of parental consent for permanent methods in the "Politique et normes" contrasts with the previous version of the policy from 2005, which did not identify permanent methods as requiring consent.
The
Loi n
2011-087 du 30 d
cembre 2011 portant code des personnes et de la famille
states that wives must obey their husbands and that husbands are the head of the family:
Article 316 : Dans la limite des droits et devoirs respectifs des e
poux consacre
s par le pre
sent Code, la femme doit obe
issance a
son mari, et le mari, protection a
sa femme
Article 319 : Le mari est le chef de famille. Il perd cette qualite
au profit de la femme en cas :
- d'absence prolonge
e et injustifie
e ;
- de disparition ;
- d'interdiction ;
- d'impossibilite
de manifester sa volonte
.
Le choix de la re
sidence de la famille appartient au mari. La femme est tenue d
habiter avec lui et il est tenu de la recevoir.
Ce choix doit se faire dans l
inte
t exclusif du me
nage.
Les charges du me
nage pe
sent sur le mari. La femme marie
e qui dispose de revenus peut contribuer aux charges du me
nage.
Mali is placed in the yellow category for this indicator as youth are unable to access permanent methods of contraception without spousal and parental consent. To improve the policy environment, policymakers should legally protect youth access to all FP services without consent from a parent or spouse.
No law or policy exists that requires providers to authorize medically advised youth FP services without personal bias or discrimination. Mali is placed in the gray category for this indicator.
The
Politique et normes des services de sant
de la reproduction, 2019
states that contraceptives should be offered to all adolescents and young people:
3.4.1 La contraception
c. B
ficiaires
Les b
ficiaires des services de contraception sont les hommes, les femmes en
ge de procr
er et en particulier les femmes jeunes sans enfant, les grandes multipares, les personnes
comportement
risque des IST [infection sexuellement transmissible], VIH et Sida, les malades mentaux, les adolescents(es) et les jeunes, la famille et la communaut
.
Therefore, Mali is placed in the green category for this indicator.
The
Loi n
02-044 relative
la sant
de la reproduction, 2002
states that all individuals and all couples are guaranteed access to reproductive health:
Article 3 : Les hommes et les femmes ont le droit
gal de libert
, de responsabilit
, d'
tre inform
s et d'utiliser la m
thode de planification ou de r
gulation des naissances de leur choix, qui ne sont pas contraires
la loi.
Article 4 : Tout individu, tout couple a le droit d'acc
der librement
des services de sant
de reproduction et de b
ficier des soins de la meilleure qualit
possible.
The
Plan d
action national budg
de planification familiale du Mali, 2019-2023
interprets the
Loi n
02-044
as a guarantee of access to contraceptives by individuals and couples:
Le pays a vot
, en juin 2002, la loi sur la sant
de la reproduction qui garantit le droit
tous les couples et aux individus de disposer d
informations et de services de qualit
en mati
re de planification familiale.
The
Plan d
action
also supports access to contraception regardless of marital status:
Les contraceptifs sont distribu
s sans distinction
toutes les femmes (mari
es ou non-mari
es)
Because Mali
s policies support access to contraceptives for unmarried individuals and couples, Mali is placed in the green category for this indicator.
The
Plan d
cennal de d
veloppement sanitaire et social, 2014-2023
affirms the need to make all methods available to youth, including long-acting reversible contraceptives (LARCs):
RS-1.3
: La planification familiale et mieux repositionn
dans les activit
s de SR [sant
reproductive]
Les interventions prioritaires retenues dans ce domaine sont les suivantes
: D
veloppement d
interventions sp
cifiques pour renforcer la continuit
de l
offre de services PF de qualit
notamment l
utilisation des m
thodes de longue dur
e, l
augmentation de la demande des services de la PF et la facilitation de l
s des femmes, des hommes, des jeunes et adolescents aux services de PF.
The
Politique et normes des services de sant
de la reproduction, 2019
also support adolescent and youth access to contraceptive methods:
c. B
ficiaires :
Les b
ficiaires des services de contraception sont les hommes, les femmes en
ge de procr
er et en particulier les femmes jeunes sans enfant, les grandes multipares, les personnes
comportement
risque des IST [infection sexuellement transmissible], VIH et Sida, les malades mentaux, les adolescents(es) et les jeunes, la famille et la communaut
.
While the policy environment is supportive of youth access to contraceptive methods, it does not explicitly state youth access to a range of methods, including LARCs, regardless of age, marital status, or parity. Therefore, Mali is placed in the yellow category for this indicator.
Although the availability of emergency contraception (EC)
is not factored into the categorization of this indicator, note that the
Politique et normes
includes EC in the general list of contraceptive methods, but not in the adolescent-specific section on sexual and reproductive health. Thus, it is not clear whether the policy intends for EC to be accessible to youth.
The
Loi n
02-044 relative
la sant
de la reproduction, 2002
guarantees information and education on contraception:
Article 12: Sont
galement autoris
es, l
information et l'
ducation concernant la contraception dans le respect de l'ordre public sanitaire et de la morale familiale.
The
Guide for Constructive Men
s Engagement in Reproductive Health 2008
describes strategies for educating youth about sexual and reproductive health in informal and formal settings:
Objective:
To increase the number of adolescents and young adults trained and sensitized in sexual and reproductive health who adopt positive behaviors within the community.
Strategies:
Develop innovative initiatives that promote RH within formal and informal education systems
Encourage sex education dialogue within the family
The
Plan d
action multisectoriel sant
des adolescents et des jeunes, 2017-2021" includes multiple school-based and out-of-school activities to increase young people
s awareness of FP information and services, including activities to build civic engagement (one of the nine essential components of comprehensive sexuality education [CSE]):
Axe strat
gique 1 : Am
lioration de l
des informations appropri
es aux besoins sanitaires des adolescents et des jeunes et mobilisation communautaire dans le processus de d
veloppement et de mise en
uvre des programmes et projets de
SAJ [sant
des adolescents et jeunes
].
Objectif sp
cifique 1 : Assurer la prise en charge globale des IST [infection sexuellement transmissible]/VIH/Sida chez 80% des adolescents et des jeunes sur toute l
tendue du territoire
- Organiser 100 journ
es de sensibilisation sur l
offre de services int
s de PF et VIH chez les jeunes dans les
tablissements scolaire et universitaire et sur les espaces de jeu.
Objectif sp
cifique 2
: Assurer l
offre des services de Planification Familiale chez 50% des adolescents et des jeunes sur toute l
tendue du territoire,
- Organiser 70300 s
ances (causeries
ducatives, d
bats) au niveau scolaire, non scolaire et universitaire sur la PF
- Organiser / sponsoriser 50 (soit 10 par an) activit
nementielles qui regroupent les adolescents et les jeunes (festival, streetball, concert, comp
tition sportive, caravane ...)
- Organiser 100 journ
es d'information et de sensibilisation sur la PF aupr
s des femmes et des leaders religieux
- R
aliser et diffuser 200 spots et 200
missions radio en faveur de la PF
Axe 4 : Implication et responsabilisation des adolescents et jeunes dans la promotion de la SAJ
Objectif sp
cifique 1 : Impliquer les adolescents et les jeunes dans la conception et la mise en
uvre des programmes et projets en faveur de la SAJ.
- Re-dynamiser 200 r
seaux des organisations d
adolescents et de jeunes du Mali.
- Harmoniser les modules de formation de sensibilisation et d'
ducation pour le changement de comportement en faveur de la SAJ.
- Organiser 250 sessions de formation
l'endroit des r
seaux de jeunes pour le renforcement de leur capacit
dans la mise en
uvre des activit
s en SAJ pr
vues dans leurs plans d'actions annuels
tous les niveaux.
- Organiser deux (02) forums nationaux sur la Sant
des adolescents et des jeunes avec le r
seau des associations
- Impliquer les organisations de jeunesses au processus d'
laboration et de mise en
uvre des plans d'actions SAJ
tous les niveaux
The
Plan d
action national budg
de planification familiale du Mali, 2019-2023
describes a specific activity to improve youth advocacy, one of the nine essential components of CSE, by strengthening partnerships with youth groups working in FP. However, this is not described as a component of a CSE program.
Other policy documents, including the "Politique et normes des services de sant
de la reproduction, 2019" and the "R
duction de la mortalit
maternelle n
onatale et infanto-juvenile: plan strat
gique, 2014-2018" support the strengthening of sexual health education for adolescents and young people.
Mali is placed in the yellow category for this indicator because its policy environment supports the provision of sexuality education, but it does not describe the components that should be included in a CSE program.
The "Plan d
action national budg
de planification familiale du Mali, 2019-2023
addresses the need for FP programs to account for youth and references a specific policy document,
Plan strat
gique de sant
et de d
veloppement des adolescents et des jeunes, 2017-2021
which aims to contribute to improving the health and development of young people through youth-friendly services. As of February 2022, this policy document could not be located for review.
The Plan d
action builds on the preceding action plan by laying out activities to train providers and the staff who train them to be more youth friendly, as well as create youth-friendly spaces with a focus on confidentiality:
Objectif prioritaire 6 : Am
liorer l
adaptation des services PF aux adolescents/ jeunes et les personnes vuln
rables
Action prioritaire 11 : Renforcement de l
s aux services PF y compris PFPP [planification familiale du post-partum] et SAA [soins apr
s avortement] des groupes vuln
rables et sp
cifiques (adolescents et jeunes, personnes vivant avec un handicap, r
fugi
s, d
plac
es, personnes vivant avec le VIH, etc.)
Activit
: Renforcer l
offre adapt
e aux besoins des adolescents et des jeunes
Sous-activit
s:
- Former 25 formateurs nationaux et r
gionaux sur la SAJ [sant
des adolescents et des jeunes]...
- Former 1 435 prestataires des districts sanitaires sur la SAJ (1 personne/74 CSRef [Centre de sant
de r
rence] et 1 personne/1 361 CSCom [Centre de sant
communautaire])...
- Am
nager des espaces (salles d'attente, confidentialit
, sortie
part) pour adolescents et jeunes dans 1 000 structures de sant
pour l'offre des services conviviaux aux adolescents et jeunes...
- Renforcer les capacit
s des 1 435 centres pour adolescents et jeunes existants pour l'offre de services conviviaux aux adolescents et jeunes...
- Int
grer dans les PMA[Paquet minimum d
actions] l'offre de services conviviaux aux adolescents et jeunes de pr
rence par les prestataires jeunes...
- R
aliser par les CSCom avec les animateurs des ONG [Organisation non gouvernementale] 2 042 (3 sorties par an pour 680 CSCom pendant 4 ans) sorties cibl
es d'offre de services
l'endroit des groupes de jeunes et adolescents (jeunes en situation de rupture familiale, etc.)
The
Plan d
action
also acknowledges that training activities will be done to reduce the stigma and discrimination faced by youth:
Des efforts programmatiques vont aussi
tre faits pour que des prestations et actes de PF deviennent accessibles financi
rement pour tous. Lesdits efforts faciliteront
galement l
un plus grand nombre de services adapt
s aux jeunes dans des structures sanitaires avec un personnel form
cet effet, r
duisant ainsi la stigmatisation et les discriminations auxquelles les jeunes font face dans certains centres.
The
Plan d
action
mentions the president
s declaration to initiate free FP services, including steps that should be taken before the policy is implemented:
O.2.2. Renforcement de l
s financier aux services de PF, y compris PFPP
Un m
canisme de suivi de la d
claration du Pr
sident de la R
publique concernant la gratuit
des contraceptifs va
tre mis en place. Des sessions de plaidoyer seront organis
es aupr
s de la pr
sidence pour assurer la mise en
uvre effective de la mesure (voir l
axe politique, environnement habilitant et financement). Pour permettre cet acc
s aux services PF, avant que la politique de gratuit
ne soit mise en
uvre, le le PANB [Plan d
action nationale budg
] pr
voit des campagnes annuelles d'intensification de l'offre de PF gratuite
tous les niveaux et les journ
es gratuites mensuelles de prestation PF dans les structures de sant
.
Il convient aussi d
laborer et de mettre en
uvre des plans d
urgence des districts affect
s par la crise avec l
offre gratuite de services dans les camps de d
plac
s ou de r
fugi
s et pour les communaut
accueils.
The
Guide for Constructive Men
s Engagement in Reproductive Health 2008
discusses confidentiality:
Objective:
To increase the number of adolescents and young adults trained and sensitized in sexual and reproductive health who adopt positive behaviors within the community.
Strategies:
Reinforce a climate of trust and confidentiality with teenagers and youth when they access RH [reproductive health] services
The
duction de la mortalit
maternelle n
onatale et infanto-juvenile
: plan strat
gique, 2014-2018
also includes an action item to improve the welcoming environment for youth when seeking RH services:
Strat
gie 3.3 : Promotion de l
approche qualit
intervention des structures Les interventions prioritaires :
- Am
liorer l
accueil dans les structures pour un acc
s facile des femmes, des hommes, des jeunes et adolescents aux services de SR
[sant
reproductive] ;
The
Plan strat
gique de s
curisation des produits de la sant
de la reproduction (SPSR), 2017-2021 au Mali
states in its objectives to make reproductive health products available and affordable to all users:
Ce plan strat
gique qui entre en
troite ligne avec les orientations strat
giques du PRODESS III, marque la volont
du Minist
re de la Sant
et de l
Hygi
ne Publique de :
- Rendre les produits SR de qualit
constamment disponibles, abordables, et accessibles aux utilisateurs ;
The
Plan d
action multisectoriel sant
des adolescents et des jeunes, 2017-2021
includes two specific objectives to increase family planning service use by adolescents and young people and to reduce incidence of undesired and teenage pregnancies. To reach those goals, the
Plan d
action multisectoriel
outlines specific activities that will help increase family planning demand, including one to train providers:
Objectif sp
cifique 2 : Assurer l
offre des services de
Planification Familiale
chez 50% des adolescents
jeunes sur toute l
tendue du territoire
Activit
:
- Former 400 prestataires des formations sanitaires et des centres jeunes pour offrir les services de PF adapt
s aux adolescents et aux jeunes.
- Assurer l
approvisionnement r
gulier de 1500 structures sanitaires par niveaux de la pyramide sanitaire en intrants de la PF en quantit
et en qualit
- Former/Recycler 100 g
rants de d
t et directeurs techniques des centres en gestion logistique des produits contraceptifs
Mali is placed in the green category for this indicator because its policies adequately address all three adolescent-friendly service-delivery elements.
The
Programme de d
veloppement socio-sanitaire, 2014-2018
includes a plan to engage parents through developing a training curriculum on communicating with adolescents about sexual and reproductive health:
Afin de promouvoir la planification familiale au Mali, le MPFFE [Minist
re de la Promotion de la Femme, la Famille et l
Enfant] se propose de sensibiliser les membres des communaut
s sur la sant
de la reproduction et la planification familiale ainsi que de diffuser la politique de la l
gislation relative
la SR [sant
de la reproduction]
Un plan int
de communication pour le repositionnement de la PF sera
labor
et un curriculum de formation des parents sur la communication avec les enfants et les ados sur la SR d
velopp
.
The
Plan d
action national budg
de planification familiale du Mali, 2019-2023
recognizes the importance of an enabling environment in access to family planning. The first strategic priority of the
Plan d
action
is to create demand, especially for young people and adolescents, by developing partnerships with the community:
Priorit
1 : Cr
er la demande aupr
s des populations, notamment chez les jeunes, les adolescents, les femmes et les hommes, y compris en contexte humanitaire, en d
veloppant un partenariat strat
gique avec les
lus locaux, les leaders communautaires et religieux.
Actions within the strategic priority to create demand include strengthening the commitment of community members
including elected officials and religious and community leaders
to support family planning and spreading awareness and building support within the broader community through dialogue and action:
CD1.1. Renforcement de l
engagement des
lus locaux, leaders religieux, communautaires en faveur de la PF
L
engagement des leaders communautaires, religieux et
lus locaux sera obtenu
travers le renforcement de leur niveau de connaissance et de leur implication en mati
re de PF (multiplication des sessions de formation et d
orientation des leaders femmes, jeunes et hommes et renforcement des contacts avec les communes en faveur de la SR/PF des jeunes). Les strat
gies suivantes seront utilis
es, telles que l
adaptation et la multiplication des outils et supports de communication sur la PF, la formation en PF, l
utilisation de l'approche Jigisigi F
te de Mariage, bas
e sur l
utilisation d
un livret donnant au couple des informations sur leur sant
en g
ral et sur leur sant
reproductive en particulier.
CD1.2. Am
lioration de la communication sur la PF
l'endroit des communaut
s
La mobilisation communautaire pour la promotion de la PF se r
alisera
travers l'implication des groupements f
minins et de jeunes/adolescents, des associations professionnelles, des municipalit
s, et des m
dias modernes et traditionnels dans les activit
s. Pour ce faire, les strat
gies suivantes seront utilis
es, notamment, le d
veloppement de partenariats avec les municipalit
s, l
organisation de campagnes nationales PF et d
autres activit
s de masse, l
utilisation d
approches comme T
rikunda J
kulu (TJ).
The
Plan d
action
also details a male engagement strategy focused on building male FP champions through peer learning and education groups:
CD1.3. Renforcement de la participation des hommes dans la promotion de la SR/PF (ECH)
L
engagement des hommes est envisag
sous trois angles :
- L
homme en tant que client des services de la SR pour lui-m
me
- L
homme en tant que partenaire de soutien au sein du couple en mati
re de reproduction
- L
homme en tant que facteur de changement au sein de la communaut
Cette strat
gie d
engagement constructif des hommes sera mat
rialis
e dans le PANB [Plan d
action nationale budg
] 2019-2023
travers les exp
riences dites de
cole des maris
clubs des maris
clubs des futurs maris
, et
approche Handarey
Finally, the Plan d
action aims to strengthen the decision-making power of women, adolescent girls, and young women in the choice and use of family planning, as well as mobilize adolescents and young people through appropriate communication.
The
Plan d
action multisectoriel sant
des adolescents et des jeunes, 2017-2021
includes multiple activities to better increase community awareness of youth family planning, including awareness days with religious leaders:
Axe strat
gique 1 : Am
lioration de l
des informations appropri
es aux besoins sanitaires des adolescents et des jeunes et mobilisation communautaire dans le processus de d
veloppement et de mise en
uvre des programmes et projets de SAJ [sant
des adolescents et des jeunes].
Objectif sp
cifique 3 : Augmenter l
utilisation des services de Planification Familiale pour les adolescents et les jeunes d
ici 2021
Activit
s
:
- Organiser 70300 s
ances (causeries
ducatives, d
bats) au niveau scolaire, non scolaire et universitaire sur la PF
- Organiser / sponsoriser 50 (soit 10 par an) activit
nementielles qui regroupent les adolescents et les jeunes (festival, streetball, concert, comp
tition sportive, caravane ...)
- Organiser 100 journ
es d'information et de sensibilisation sur la PF aupr
s des femmes et des leaders religieux 4. R
aliser et diffuser 200 spots et 200
missions radio en faveur de la PF
Mali
s policy environment adequately addresses gender norms and describes activities for engaging the community to support youth access to FP. Therefore, Mali is placed in the green category for this indicator.
The
Plan d
action national budg
en faveur de l
espacement des naissances de la Mauritanie, 2019-2023
acknowledges the difficulty young people face in discussing FP with their parents. However, no law or policy exists that prohibits parental or spousal consent for youth access to FP services. Mauritania is placed in the gray category for this indicator.
The
Plan d
action national budg
en faveur de l
espacement des naissances de la Mauritanie, 2019-2023
acknowledges the issue of provider stigma toward youth seeking FP services:
Deuxi
mement, l
offre de services de PF est inadapt
e aux adolescents et les jeunes. Le personnel soignant des centres ne sait pas comment les recevoir. On peut citer en exemple le manque de confidentialit
et m
me parfois des jugements s
res de la part du personnel des centres. De plus, quand l
offre de service de PF ne fait pas d
faut c
est l
s, que ce soit au niveau g
ographique ou financier, surtout pour les adolescents et les jeunes en situation de vuln
rabilit
.
However, no law or policy exists explicitly stating that providers must avoid discrimination or bias toward youth. Mauritania is placed in the gray category for this indicator.
The
Projet de loi
relative
la sant
de la reproduction, 2017
states that all individuals, including adolescents, are equal in dignity and rights related to reproductive health; it also prohibits discrimination based on age:
Article 7
Tous les individus, y compris les adolescents et les enfants, tous les couples sont
gaux en droit et en dignit
en mati
re de sant
de la reproduction.
Le droit
la sant
de la reproduction est un droit universel fondamental garanti
tout
tre humain, tout au long de sa vie.
Aucun individu ne peut
tre priv
de ce droit dont il b
ficie sans discrimination aucune fond
e sur l
ge, le sexe, la fortune, la couleur, la religion, l
ethnie, la situation matrimoniale ou sur toute autre situation.
Mauritania is placed in the green category for this indicator.
The
Projet de loi
relative
la sant
de la reproduction, 2017
states that all individuals, including adolescents, are equal in dignity and rights related to reproductive health (RH) and prohibits discrimination based on marital status:
Article 7
Tous les individus, y compris les adolescents et les enfants, tous les couples sont
gaux en droit et en dignit
en mati
re de sant
de la reproduction.
Le droit
la sant
de la reproduction est un droit universel fondamental garanti
tout
tre humain, tout au long de sa vie.
Aucun individu ne peut
tre priv
de ce droit dont il b
ficie sans discrimination aucune fond
e sur l
ge, le sexe, la fortune, la couleur, la religion, l
ethnie, la situation matrimoniale ou sur toute autre situation.
As the law protects youth access to RH regardless of marital status and includes FP as a component of RH services, Mauritania is placed in the green category for this indicator.
The
Projet de loi
relative
la sant
de la reproduction, 2017
includes
family planning/birth spacing
among reproductive health care services. The
Projet de loi
states that all people, including adolescents, must receive information and education on all methods of birth spacing:
Article 9
Tout couple, toute personne y compris les adolescents et les enfants, a droit
information,
ducation concernant les avantages, les risques et l
efficacit
de toutes les m
thodes d
espacement des naissances.
While the law guarantees information and education on all methods of birth spacing, it does not guarantee youth access to a range of contraceptive methods, including long-acting reversible contraceptives (LARCs).
Further, the
Guide de planification familiale
espacement des naissances,
dition r
e en avril 2008,
which includes protocols for providing each contraceptive method, states that oral contraceptives are the best method for adolescents and that intrauterine devices (IUDs) should be avoided:
4. AUTRES FEMMES A RISQUE
Adolescente : la contraception orale constitue la meilleure m
thode ; conseiller
galement l'utilisation du pr
servatifs si partenaires multiples et
viter surtout le DIU
[dispositif intra-ut
rin].
Future updates to the document should align with the World Health Organization medical eligibility criteria for contraceptive use. A more recent document,
Guide de la pratique sage-femme en Mauritanie, 1
dition, 2014,
states that IUDs and implants are acceptable for young women, and that IUDs are acceptable for nulliparous women:
Plusieurs
tudes ont d
montr
que les m
thodes contraceptives de longue dur
e sont plus efficaces que celles de courte dur
e.
Le DIU et l
implant sont donc des m
thodes contraceptives int
ressantes, m
me pour les jeunes femmes. Contrairement
une certaine id
e re
ue, le DIU n
est pas uniquement indiqu
chez les femmes ayant eu un enfant.
The
Plan d
action national budg
en faveur de l
espacement des naissances de la Mauritanie, 2019-2023
looks to improve access to a varied and comprehensive range of contraceptive methods,
with an emphasis on young people:
3.3.1. Objectifs strat
giques
Objectif 2 : Garantir la couverture en offre de services de PF] /EN [espacement des naissances] et l
s aux services de qualit
en renfor
ant la capacit
des prestataires publics, priv
s et communautaires et en ciblant les jeunes ruraux et les zones enclav
es avec l
largissement de la gamme des m
thodes y compris la mise
chelle des MLDA [m
thodes
longue dur
action] et PFPP [planification familiale du post-partum], l
lioration des services et prestations adapt
s aux besoins des jeunes.
Despite the two recent documents that take a more favorable approach to method choice for youth, the policy environment does not consistently guarantee access to a full range of methods for youth. Mauritania is placed in the red category for this indicator.
Although the availability of emergency contraception (EC) is not factored into the categorization of this indicator, note that EC is included in the 2008
Guide de planification familiale
, but it is not included in the recommended methods for youth. The 2014
Guide de la pratique
does not include EC because it focuses on LARC methods.
Mauritania
s policies support the provision of sexuality education for youth. The "Plan d
action national budg
en faveur de l
espacement des naissances de la Mauritanie, 2019-2023" prioritizes the implementation of a comprehensive sexuality education (CSE) approach for adolescents and young people in formal and informal education settings:
CD2.1. Mise en place d
une approche d
Education Compl
la Sexualit
(ECS) pour les adolescents et les jeunes non/d
scolaris
s (en situation de vuln
rabilit
).
L
ducation compl
la sexualit
permet aux adolescents et aux jeunes de prendre des d
cisions concernant leur sexualit
en connaissance de cause. Elle est dispens
e sur plusieurs ann
es et fournit aux jeunes des informations adapt
leur
ge et correspondant au d
veloppement de leurs capacit
s : des informations scientifiques et acad
miques concernant le d
veloppement humain, l
anatomie et la grossesse, mais
galement des renseignements sur la contraception et les infections sexuellement transmissibles (IST), notamment le VIH. Au-del
de leur caract
re purement informatif, ces programmes favorisent
galement la confiance ainsi qu
une meilleure communication. Ils doivent en outre traiter des questions sociales qui entourent la sexualit
et la procr
ation, notamment les normes sociales, la vie de famille et les relations humaines. En prenant en compte les r
sultats du diagnostic, il s
agit de mieux int
grer les questions de SSR [sant
sexuelle et reproductive] et autres sp
cificit
s des adolescent(e)s et des jeunes
travers les enseignements formel et non formel. L
intensification de l
enseignement de la SSR/PF dans les
coles de base doit
tre faite
travers la mise
jour des modules de formation des enseignants et la r
vision des curricula destin
s aux
ves. Les enseignants exp
riment
s seront form
s pour
tre des formateurs. Ces groupes de formateurs animeront des sessions de formation des enseignants au cours plusieurs sessions par an. Les enseignants form
s travailleront avec les
ves sur des questions de la SSR/PF en utilisant les modules r
s. Des d
pliants comportant les messages essentiels seront
labor
s pour les
ves.
However, the
Plan d
action
only partially addresses the nine essential components of CSE as defined by the United Nations Population Fund (UNFPA). Mauritania is placed in the yellow category for this indicator.
Mauritania
s policy environment acknowledges the importance of youth-friendly sexual and reproductive health (SRH) services. The
Programme national de sant
de la reproduction : projet de plan d
action, 2007
includes specific activities to pilot and study the feasibility of youth-friendly SRH services. The
Programme national de sant
de la reproduction : plan strat
gique SR, 2008-2012
aims to increase the supply of youth-friendly SRH services. It addresses training providers on specific communication techniques with youth and offering youth certain FP methods (condoms, pills, and emergency
contraception):
RESULTAT ATTENDU 2: L
offre et l
utilisation des services de SSRAJ [sant
sexuelle et reproductive des adolescents et des jeunes] est augment
ACTIONS 2
- Former les prestataires en techniques sp
cifiques de communication avec les A et J [adolescents et jeunes]...
- Faciliter l
s des AJ
la contraception (m
thodes adapt
es (pr
servatif, pilule, contraception d
urgence
)
The
Plan d
action national budg
en faveur de l
espacement des naissances de la Mauritanie, 2019-2023
includes a specific activity to train providers to offer youth-friendly services:
OA1.4. Renforcement des capacit
s des prestataires des FS [formation sanitaire] dans l'acc
la contraception et les services adapt
s de SRAJ [sant
reproductive des adolescents et des jeunes] aux adolescents et aux jeunes mari
s. Renforcer les capacit
s des prestataires des PPS [point de prestations de services] dans le domaine de l
offre des services de PF adapt
s aux adolescents et aux jeunes permettra d
accro
tre l
utilisation des services de PF/contraception des adolescents et des jeunes dans les PPS car ceux-ci seront mieux adapt
leurs besoins sp
cifiques. Elle sera r
alis
travers la formation, l
nagement des structures de soins, la supervision et le suivi des prestations
The
Plan d'action
also outlines an activity to provide free contraceptives on
family planning days
and includes a priority action to continuously advocate for free FP, particularly for adolescents and young people:
P3.5. Plaidoyer aupr
s des d
cideurs pour la gratuit
des services de PF en particulier chez les adolescents et les jeunes de 2019
2023. Au cours des activit
s de journ
es sp
ciales de PF, les m
thodes modernes de PF sont offertes gratuitement et les clientes sont souvent nombreuses, d
passant les objectifs fix
s par les services de sant
et autres prestataires. Cet
tat de fait soutient que les co
ts des produits constituent une barri
re importante
utilisation des services et produits contraceptifs dans les FS. Ces co
ts peuvent varier d
une structure
une autre. Le plaidoyer sera fait pour viser la gratuit
finitive des produits contraceptifs comme c
est le cas lors des journ
es sp
ciales PF. Il sera constitu
une
quipe de plaidoyer, un plan de plaidoyer doit
tre
labor
ainsi qu
un suivi r
gulier de la mise en
uvre du plan. Ce plaidoyer sera renforc
pour la gratuit
de la PF pour les adolescentes et les jeunes qui sont davantage concern
es par les barri
res financi
res
However, because the policies do not connect provider training to issues of judgment and do not address audio/visual confidentiality and privacy, Mauritania is placed in the yellow category for this indicator.
The
Programme national de sant
de la reproduction : projet de plan d
action, 2007
includes among its sexual and reproductive health (SRH) goals for youth a briefly described activity to reach out to leaders and to mobilize the community:
2.4 D
velopper des actions de plaidoyer aupr
s des autorit
s et des leaders et de mobilisation sociale au niveau de la communaut
The
Programme national de sant
de la reproduction : plan strat
gique, SR 2008-2012
aims to promote adolescent SRH among political, religious, and traditional leaders:
Plaidoyer aupr
s des leaders politiques, religieux, traditionnels pour la promotion de la SR [sant
de la reproduction] des A et J [adolescents et jeunes]
The adolescent SRH goals within the
Programme national de sant
de la reproduction : plan strat
gique
include an action to address age at first marriage and harmful traditional practices. However, detail is not provided beyond that action.
The
Plan national de d
veloppement sanitaire, 2017-2020
aims for all health facilities to provide a minimum package of youth and adolescent reproductive health services through involvement with community actors:
3.2.3. Sant
de l
adolescent et du jeune
Acc
quitable des adolescentes et des jeunes aux services cliniques et d
information de qualit
:
Un paquet minimum d
activit
s SRAJ [sant
reproductive des adolescents et des jeunes] sera assur
par tous les CS [centres de sant
] en collaboration avec les acteurs communautaires, en particulier les associations de jeunes et les ONG [organisation non gouvernementale] engag
s dans la sant
des adolescents et des jeunes.
Des centres de prise en charge des violences
gard des jeunes femmes et des adolescents seront mis en place progressivement au niveau des structures de r
rence en commen
ant par les h
pitaux.
L
implication des acteurs communautaires
travers des accords de partenariats formalis
permettra d
assurer du programme cibl
de SRAJ adapt
s aux sp
cificit
s et aux besoins des jeunes et des adolescents en zones rurales et p
riurbaines.
The
Plan d
action national budg
en faveur de l
espacement des naissances de la Mauritanie, 2019-2023
aims to provide an enabling environment for family planning through interaction with political and community leaders:
Objectif 4 : Garantir un environnement favorable pour la PF
travers :
- Le renforcement des activit
s de plaidoyer aupr
s des d
cideurs (Pr
sident de la R
publique de Mauritanie, Premier Ministre, Institutions nationales, minist
re de la sant
et minist
res connexes) et des leaders administratifs, traditionnels, religieux et des
lus.
Within its priority actions, the
Plan d'action
also targets men and community leaders as family planning advocates. The constructive engagement approach looks to build FP champions through training:
CD3.1. Mise en
uvre de la strat
gie de l
engagement constructif des hommes (ECH) dans le curriculum de la PF/EN [espacement des naissances].
engagement des hommes est envisag
selon trois axes :
- Homme en tant que client des services de la SR [sant
reproductive] pour lui-m
me
- Homme en tant que partenaire de soutien au sein du couple en mati
re de reproduction
- Homme en tant facteur changement au sein de la communaut
.
Cette strat
gie d
engagement constructif des hommes va soutenir et amplifier celle en cours dite de
cole des maris
Cette strat
gie responsabilise mieux la communaut
dans la r
solution des probl
mes li
la SR. L
approche
maris mod
les
quant
elle fait r
rence aux
poux qui accompagnent leurs
pouses aux services de sant
, les soutiennent pour l
auto prise en charge pendant la p
riode p
rinatale, sensibilisent d
autres
poux et recherchent des solutions pour l
s aux soins
CD3.2. Formation et implication des leaders religieux et coutumiers sur les outils de plaidoyer et les droits
la sant
en faveur de la SR/PF.
Etant donn
que les leaders religieux, les chefs de villages et notables constituent des d
cideurs et leaders d
opinion influents capables d
appuyer les efforts de promotion de la PF, il y a lieu de former de nouveaux champions parmi eux pour conduire en leur direction un plaidoyer soutenu en vue d
accro
tre leur engagement en faveur de la PF et les mettre
contribution dans la mobilisation des communaut
s
While Mauritania
s policy documents include plans to engage community members in supporting family planning and address gender norms, there is no detailed strategy for building an enabling social environment for youth FP specifically. Mauritania is placed in the yellow category for this indicator.
The
National Reproductive Health Commodity Security Strategy, 2015
confirms access to permanent contraceptives without spousal consent:
Contraceptives such as condoms, injectables, oral pills and other RH [reproductive health] commodities are included in Essential Drug List (EDL). There is no barrier as such in terms of age and parity for clients to access contraceptives. No prescription is required to purchase contraceptives (condoms, pills, and injectables) in the market i.e. pharmacies
Spousal consent is not required to obtain a permanent method of family planning.
The
National Adolescent Health and Development Strategy 2075, 2018
also discusses the role of parental consent when it comes to adolescent privacy and confidentiality when accessing integrated services:
Integrated services will be delivered to adolescents focusing on the following points based on primary health care:
Privacy: Ensure privacy and confidentiality
of adolescents
with none or minimal parental consent.
While the
National Family Planning Costed Implementation Plan, 2015-2020
aims to ensure that women and girls exercise informed choice when using FP, it does not specifically address consent from a third party.
While Nepal
s policies protect access to permanent contraceptives without spousal consent and acknowledge adolescents
right to services with minimal or no parental consent, they do not clearly protect youth access to all methods without consent from a third party. Nepal is placed in the gray category for this indicator.
The
National Adolescent Health and Development Strategy 2075, 2018
discusses strategies and potential actions the government should take to reach improved sexual and reproductive health knowledge, perception, and behavior. To make contraceptives available to adolescents and youth, the Strategy proposes nonjudgmental services:
Ensure non-judgmental and non-discriminatory services in private sector, health facilities and pharmacies
While the Strategy supports the need for providers to avoid judgment and discrimination, it does not require providers to authorize medically advised FP services. Nepal is therefore placed in the gray category for this indicator.
The
National Family Planning Costed Implementation Plan, 2015-2020
states that access to FP services is a human right and should be provided without discrimination and coercion. The
Safe Motherhood and Reproductive Health Rights Act, 2018
reiterates the right of every person, including adolescents, to reproductive health.
- Right to reproductive health:
(1)
Each woman and adolescent shall have the right to obtain
education, information, counseling and service relating to sexual and reproductive health.
...
(4)
Each person shall have the right to contraceptive information and usage.
The
National Reproductive Health Commodity Security Strategy, 2015
states that there are no age restrictions to the contraceptives included in the essential drug list:
Contraceptives such as condoms, injectables, oral pills and other RH [reproductive health] commodities are included in Essential Drug List (EDL). There is no barrier as such in terms of age and parity for clients to access contraceptives.
The
National List of Essential Medicines, 2021
covers a wide range of contraceptives, including oral pills, injectables, intrauterine devices, barrier methods, and implants. Nepal is placed in the green category for this indicator.
The
National Family Planning Costed Implementation Plan, 2015-2020" states that access to FP services is a human right and should be provided without discrimination and coercion.
Without a provision that explicitly protects youth access to FP services regardless of marital status, Nepal is placed in the gray category for this indicator.
The
National Adolescent Health and Development Strategy 2075, 2018
includes multiple activities to fulfill adolescents
contraceptive needs, some of which reference access to long-acting reversible contraceptives (LARCs):
Strategy: Fulfill unmet needs and requirements of adolescents
and ensure quality contraceptive services.
- Provide counseling on selection of appropriate contraceptive methods
- Provide quality contraceptive services including emergency contraception in both public and private health facilities through trained service providers
- Provide counseling services on clinical contraceptive devices such as intrauterine contraceptive devices (IUCDs) according to the protocol
- Raise awareness and provide counseling on dual protection usage of condoms and increase accessibility
- Include and visibly list family planning/ contraceptive services especially for newly married adolescents when organizing mobile health camps for adolescents.
The
National Reproductive Health Commodity Security Strategy, 2015
states that there are no age restrictions to contraceptives included in the essential drug list:
Contraceptives such as condoms, injectables, oral pills and other RH commodities are included in Essential Drug List (EDL). There is no barrier as such in terms of age and parity for clients to access contraceptives.
The
National List of Essential Medicines Nepal, 2021
covers a wide range of contraceptives, including oral pills, injectables, intrauterine devices, barrier methods, and implants, but does not note any eligibility criteria for the methods.
However, while Nepal
s policies are promising in that they acknowledge no age or parity restrictions to contraceptive access, they do not explicitly mention youth
s legal right to access a full range of contraceptive services, including LARCs. Nepal is therefore placed in the gray category for this indicator.
Although the availability of emergency contraception (EC) is not factored into the categorization of this indicator, it is worth noting that Nepal
s policies do not explicitly specify whether access to ECs should be available to adolescents.
The
Nepal Safe Motherhood and Newborn Health Roadmap, 2030
recognizes the importance of a comprehensive sexual and reproductive health (SRH) education at schools:
Given the high enrolment rates in primary schools in Nepal and gender parity in enrolment, another key opportunity to provide accurate and relevant information is Sexual and Reproductive Health (SRH) education at schools. SRH education and life skills education should be comprehensive, including covering risks of adolescent pregnancy, and MoHP [Ministry of Health and Population] should continue to advocate that it is made compulsory for both boys and girls.
The
Nepal Health Sector Strategy Implementation Plan, 2016-2021
includes key interventions to incorporate comprehensive sexuality education (CSE) in school curricula:
- Comprehensive sexuality education incorporated in school curriculum
- Develop and implement curriculum for school-based health education (include mental health, ayurveda, nutrition, sexual and reproductive health, gender-based violence)
.
- Update school curricula on Comprehensive Sexuality Education (CSE) in line with ITGSE [International Technical Guidance on Sexuality Education] (in coordination with MoE [Ministry of Education]) and also develop text book accordingly with capacity building of the teachers
The key interventions listed in the
National Family Planning Costed Implementation Plan, 2015-2020" provide further details on CSE:
Support integration and implementation of Comprehensive Sexuality Education (CSE) in schools secondary and higher level. Support will be provided to fully implement CSE curriculum in grades 6-10 and interactive sessions with students in grades 11-12 will be conducted. It will include advocacy with the Ministry of Education, training of educators/teachers and updating teaching materials and other communication tools.
The Costed Implementation Plan also includes interventions that reach across formal and informal sectors to improve youth access to contraceptive information and services:
Design, implement and evaluate special programme to increase access and utilization of FP among adolescents and young people. To support access to contraceptives information and services among adolescents and young people, a peer education programme will be developed and implemented both in- and out-of school.
.
3. Reach adolescents with FP messages through innovative approaches (m-health & e-health)
3.1 Utilize SMS technology to promote FP use amongst adolescents/youth
3.2 Introduce FP messages through mobile health apps
3.3 Implement hotline telephone program for adolescents
3.4 Pilot & implement e-health FP program for adolescents in urban areas
.
7.1 Develop age-specific peer education program (both in-school and out-of-school youth)
7.3 Integrate FP into school health programme (no additional costs)
The
National Adolescent Health and Development Strategy 2075, 2018
outlines a strategic objective and possible actions to improve SRH knowledge and promote CSE:
- To improve knowledge, perception and behaviors of sexual and reproductive health and promote comprehensive sexuality education through extensive collaboration with education sector;
.
Review and revise curriculums of lower secondary and secondary level and focus on behavioral and emotional changes that occur during adolescence and other matters related to adolescent health and development as well as matters identified by adolescents themselves in order to encourage dialogue and debate on adolescent sexual and reproductive health and healthy lifestyle
Although the Strategy does not provide specific details on a CSE curriculum, it briefly touches on the need to provide safe sex information in schools:
2.1 To improve knowledge, perception and behavior related to sexual and reproductive health
Promote responsible sexual behavior.
Provide counseling on masturbation, sexual abstinence before marriage and safe sex, if needed, through health facilities, adolescent-friendly information corner in schools or peer groups.
The Strategy also notes the importance of including topics on sexual abuse and gender-based violence in the school curriculum:
Help improve school curriculum (about teen safety, domestic violence, and child protection) for developing skills and knowledge about sexual abuse and gender violence/abuse and possible safety measures.
Nepal
s policy environment is promising as it focuses on SRH education and awareness-raising activities for youth, but it does not address all nine UNFPA essential components. Nepal is therefore placed in the yellow category for this indicator.
The
Nepal Health Sector Strategy Implementation Plan, 2016-2021
outlines the program components of the Family Health Division within the Ministry of Health and Population, and notes that the key function of the Adolescent Sexual and Reproductive Health department is to create an adolescent-friendly environment:
Create a conducive environment in public health facilities for adolescents to access adolescent reproductive health services.
The Implementation Plan also includes an activity to train service providers on adolescent sexual and reproductive health to improve availability of human resources, with a focus on rural retention and enrollment:
Train services provider on ASRH [adolescent sexual and reproductive health] basic (5 day) package from Adolescent Friendly Service Sites/Centres
Create a conducive environment in public health facilities for adolescents to access adolescent reproductive health services
The
National Adolescent Health and Development Strategy 2075, 2018
notes that the Ministry of Health and Population introduced the five-day Adolescent Sexual and Reproductive Health Training Package in 2015. Health facilities have started to implement and monitor adolescent-friendly services although details of the adolescent-friendly certification requirements could not be accessed for review. The strategy includes training providers under its objective to create a safe and supportive environment:
Provide orientation and training on National Adolescent Sexual and Reproductive Health and adolescent-friendly services to service providers of all health facilities.
The Strategy notes that adolescent-friendly services should provide nonjudgmental services to improve sexual and reproductive health knowledge, perception, and behavior:
Ensure non-judgmental and non-discriminatory services in private sector, health facilities and pharmacies.
The Strategy also discusses the role of parental consent when it comes to adolescent privacy and confidentiality when accessing integrated services, but is not specific to family planning:
Integrated services will be delivered to adolescents focusing on the following points based on primary health care:
.
Privacy: Ensure privacy and confidentiality of adolescents with none or minimal parental consent.
The
Safe Motherhood and Reproductive Health Rights Act, 2018
requires that individuals accessing reproductive health services and information also receive confidentiality. In addition, the Act states that each person has the right to affordable reproductive health services.
Furthermore, the
National Family Planning Costed Implementation Plan, 2015-2020
and
National Reproductive Health Commodity Security Strategy, 2015
confirm that FP services have been integrated into the reproductive health package as a basic health service and are now provided free of charge to the entire population at government facilities. In addition to free contraceptives, the government provides a nominal wage compensation for permanent methods.
While Nepal
s policy environment discusses the implementation of adolescent-friendly services, it provides no details on what these services entail and whether spaces and providers will ensure non-judgmental services with confidentiality and privacy. As Nepal
s policies confirm free contraceptives, it is placed in the yellow category for this indicator.
The
National Family Planning Costed Implementation Plan, 2015-2020" includes an intervention to address sociocultural barriers for youth access to FP services, including involving key stakeholders at the district and community levels:
Strategic Action Area: Enabling Environment
A policy environment that enables the above four Action Areas to be implemented effectively is key for a successful FP programme. Strategic interventions in this area include increasing advocacy at all levels for FP; addressing legal and socio-cultural barriers to young people accessing FP; strengthening the integration of services; and developing/updating national polices and strategies to facilitate task shifting. Estimated resources required to implement the key interventions are presented in Annex C.
Key Interventions:
- Increase Advocacy for Family Planning. Identify national champions for FP from multiple fields and support them to advocate for FP by providing advocacy materials/tools and conducting follow up meetings. Develop and distribute advocacy packages using global evidences and tools, including modeling exercises, (in English and Nepali) for key stakeholders. Support high level advocacy events at central level and districts engaging parliamentarians, governmental officials and donors as well as civil society organizations and media. Support advocacy events at community level including celebration of FP day at community level.
Under the strategic action to increase demand for contraceptives, the Costed Implementation Plan also includes an activity to reduce misconceptions around FP methods in communities:
Reduce fear of side effects, myths and misconceptions about FP through various communication channels. Support development of [information, education, and communication] materials that emphasize value of daughters and clarify information about modern contraceptives to be used by [female community health volunteers], health workers and community leaders. Organize forums and interactive sessions on clients
satisfaction in communities.
The
National Adolescent Health and Development Strategy 2075, 2018
includes a strategic objective to create a supportive social environment to promote reproductive health:
Strategy: Raise awareness about safe reproductive and sexual behaviors in community and family
Possible actions:
- Organize discussion/debate on reproduction related problems faced by adolescents
- Organize health camps and provide orientation/counseling services related to adolescent sexual health in schools
The Strategy also discusses how adolescent health programs should identify and address
the special gender needs of adolescents
in a fair and non-discriminatory manner to ensure gender equity. It identifies multiple actions that can be taken to address gender norms in the community:
- Increase public awareness about different types of violence including gender violence by developing IEC materials
- Increase public awareness about laws and punishments related to gender violence, forced marriage, child marriage, and domestic violence.
- Organize adolescent-targeted gender violence programs.
While Nepal
s policies detail strategies and possible actions to create an enabling environment for FP access for youth, they do not include steps to address gender norms specific to youth FP. Nepal is placed in the yellow category for this indicator.
None of the policy documents reviewed for Niger include language addressing parental or spousal consent. The lack of policy language supporting youth access to FP services without these authorizations creates a potential barrier for youth in Niger interested in accessing contraception. To improve the policy environment, policymakers should consider including specific provisions for youth to access FP services without consent from a parent or spouse. Niger is placed in the gray category for this indicator.
Niger
s policy environment does not address provider authorization. Niger is placed in the gray category for this indicator.
Nigerien law recognizes the rights of all people to receive sexual and reproductive health care broadly. Article 2 of the
Loi sur la sant
de la reproduction au Niger, 2006
acknowledges that reproductive health is a universal human right and should be free from discrimination, including discrimination based on age or marital status:
Article 2 - Caract
re universel du droit
la sant
de la reproduction. Tous les individus sont
gaux en droit et en dignit
en mati
re de sant
de la reproduction. Le droit
la sant
de la reproduction est un droit universel fondamental garanti
tout
tre humain, tout au long de sa vie, en toute situation et en tout lieu. Aucun individu ne peut
tre priv
de ce droit dont il b
ficie sans discrimination aucune fond
e sur l'
ge, le sexe, la fortune, la religion, l'ethnie, la situation matrimoniale ou sur toute autre situation.
Niger is placed in the green category for this indicator.
While the
Loi sur la sant
de la reproduction au Niger, 2006
makes a declarative statement supporting the rights of all people, regardless of age or marital status, to receive reproductive health care, the following article emphasizes the right of legally married couples to reproductive health:
Article 2 - Caract
re universel du droit
la sant
de la reproduction
Tous les individus sont
gaux en droit et en dignit
en mati
re de sant
de la reproduction. Le droit
la sant
de la reproduction est un droit universel fondamental garanti
tout
tre humain, tout au long de sa vie, en toute situation et en tout lieu. Aucun individu ne peut
tre priv
de ce droit dont il b
ficie sans discrimination aucune fond
e sur l'
ge, le sexe, la fortune, la religion, l'ethnie, la situation matrimoniale ou sur toute autre situation.
Article 3
Autod
termination
Les couples et les individus ont le droit de d
cider librement et avec discernement des questions ayant trait
la sant
de la reproduction dans le respect des lois en vigueur, de l'ordre public et des bonnes m
urs. Les couples l
galement mari
s peuvent d
cider librement et avec discernement de l'espacement de leurs naissances et de disposer des informations n
cessaires pour ce faire, et du droit d'acc
der
la meilleure sant
en mati
re de reproduction.
Additionally, while the
Planification familiale au Niger : plan op
rationnel, 2018
acknowledges that the use of contraceptive methods by young unmarried women is negatively perceived by the public, it states that such a perception does not align with the country
s vision for adolescent and youth sexual and reproductive health. However, the
Planification familiale au Niger
plan op
rationnel
does not offer any further details:
La jeune femme c
libataire utilisant une m
thode contraceptive est mal vue par la population ce qui est contraire
la vision SSRAJ (sant
sexuelle et reproductive des adolescents et des jeunes) ;
This emphasis on legally married couples stands in contrast to the rest of the law, which extends reproductive rights, including FP, to all individuals. To address this discrepancy, the government should clarify policy language supporting access to FP services by married and unmarried couples and individuals, including youth. Furthermore, the government should provide specific policy language regarding its vision for adolescent and youth sexual and reproductive health, and particularly the right of young unmarried women to access and use contraceptive methods. Niger is placed in the yellow category for this indicator.
Niger
s policy environment does not discuss extending access to a full range of family planning methods to youth. Niger is placed in the gray category for this indicator.
Activity 1.1.19 of the
Planification familiale au Niger : plan d
action, 2012-2020
briefly references strengthening FP education for high school students through the home economics curriculum.
Renforcer l'enseignement de la PF au cours d'
conomie Familiale dans les CES [coll
ges d
enseignement secondaire].
Recognizing the need for FP education demonstrates a level of policy commitment on this issue. However, the policy fails to include specific guidelines on the content of the material and how the lessons should be instructed, nor coverage for young people outside of this specific course.
One of the demand-generation objectives of the
Planification familiale au Niger : plan op
rationnel, 2018
aims to reinforce the adolescent and youth family
life education program.
Objectif CD 3 : Renforcer le programme d'
ducation
la vie familiale des adolescents et jeunes
D
finition de l
Objectif : La majorit
des adolescents et jeunes n
ont pas d
informations pr
cises et approfondies sur les questions de procr
ation et de pr
paration
la gestion future de la vie familiale. Le MSP [Minist
re de la sant
publique] va travailler
parer les adolescents et jeunes
la parent
responsable. Il formera les adolescents et jeunes
travers les canaux propices (mise
chelle de la formation sur les curricula en milieu scolaire, etc.). Il les sensibilisera dans les villages, au niveau des centres de promotion des jeunes, les
Makarantas
les Fada
, les centres de formation des jeunes pour apprendre et discuter de la PF.
The 2018
Plan
offers more details about program approach than the 2012-2020
Plan.
Examples of such details include a focus on preparing adolescents and youth for responsible parenting and a mention of implementation of activities in settings outside of schools (such as villages, youth promotion centers, and youth training centers). However, the policy lacks content specificity and directives for instruction.
Niger
Plan strat
gique sectoriel de mise en
uvre de la politique nationale de jeunesse, 2011-2015
discusses several actions to raise youth awareness and use of sexual and reproductive health services, including supporting sexuality education through peer education using adapted training modules:
ACTION 22 : Appui
instauration de l
ducation sexuelle au sein de la famille et des groupes de jeunes :
La strat
gie d
ducation par les pairs sera promue dans les quartiers, les villages, hameaux, les
coles, les structures informelles de regroupement des jeunes pour toucher le maximum des cibles (parents comme jeunes) sur la base de modules de formation adapt
s qui seront d
finis, test
s, appliqu
s et
valu
s tout le long du processus.
As the reviewed policy documents do not reference all nine of the United Nations Population Fund
s (UNFPA
s) essential components of comprehensive sexuality education (CSE), Niger is placed in the yellow category for this indicator.
The
Planification familiale au Niger : plan op
rationnel, 2018
identifies youth as a priority population and includes a service access objective targeting youth.
Objectif AS 2 : Augmenter les points d
s aux services de SR [sant
reproductive] /PF pour les adolescents et jeunes en milieux scolaire et extrascolaire.
D
finition de l
Objectif : Les jeunes ont des besoins sp
cifiques en mati
re de planification familiale qui ne sont pas suffisamment pris en compte alors qu
ils sont plus expos
des pratiques
risque en mati
re de sant
sexuelle et de reproduction. Le MSP [minist
re de la Sant
publique] cherche
accro
tre la disponibilit
de points d
s aux services de planification familiale adapt
leurs besoins. Il renforcera davantage les capacit
s des prestataires en approche jeunes
tous les niveaux pour offrir aux jeunes et aux adolescents, des services de planification familiale et des soins de sant
de la reproduction de qualit
.
The
Plan de d
veloppement sanitaire, 2017-2021
aims to strengthen the supply of health services for young people and adolescents by integrating youth health services into all levels of the health system:
Poursuivre l
gration des services de sant
des jeunes dans les paquets des services
tous les niveaux du syst
me de sant
gration des services de sant
des jeunes et des adolescents dans les paquets d
activit
tous les niveaux du syst
me de sant
va se poursuivre pour augmenter la disponibilit
et la capacit
des services. Les interventions qui seront cibl
es sont : la prise en charge des infections sexuellement transmissibles, le d
pistage volontaire du VIH, le d
pistage volontaire de la dr
panocytose, la pr
vention de la grossesse (disponibilit
des produits contraceptifs), la prise en charge des cons
quences de l
avortement, etc.
Collaborer avec les jeunes afin de d
finir les strat
gies et interventions d
offre de services adapt
leurs besoins ;
Both policy documents highlight the government
s commitment to increasing the availability of FP service access points tailored to the needs of youth and indicates that building the capacity of service providers in a
youth approach
will be prioritized.
Multiple news sources reference a 2007 law that guarantees free access to contraceptive methods to all women in all public facilities. In the absence of a review of the policy document, it is unclear whether youth are identified as beneficiaries. However, the reviewed policies do not mention enforcing confidentiality and audio/visual privacy or connect provider training to judgment issues. Because the policies do not adequately cover all three of the service-delivery elements of youth-friendly FP services, Niger is placed in the yellow category for this indicator.
The
Plan strat
gique sectoriel de mise en
uvre de la politique nationale de jeunesse, 2011-2015
lays out sensitization activities to target parents and community leaders about teenage pregnancy and adolescent development. While the activities are part of a larger strategic plan that includes promotion of youth sexual and reproductive health and rights, these activities do not specifically target youth FP:
ACTION 15 : Sensibilisation aux cons
quences n
fastes des grossesses pr
coces et rapproch
es
La persistance des grossesses pr
coces et rapproch
es reste encore tr
s pr
occupante et, est li
une insuffisance d
information sur les cons
quences de ces pratiques.
. Elles cibleront aussi bien les jeunes que leurs parents, les leaders d
opinion et les d
cideurs politiques. La mise en
uvre se fera
travers l
organisation des causeries
ducatives, des pr
ches, des caravanes, des journ
es de plaidoyer, la diffusion des spots radio t
s, des sketchs, la tenue de th
tre forum.
ACTION 19 : Renforcement des capacit
s des parents sur la parent
responsable et la gestion de l
adolescence
La gestion de l
adolescence constitue une p
riode critique au cours de laquelle les parents ont des difficult
s pour encadrer leurs enfants. Deux campagnes de sensibilisation et d
information seront men
es chaque ann
e dans chaque commune du pays en vue d
atteindre l
objectif de deux millions six cent cinquante (2.650.000) personnes sur l
importance de la parent
responsable et la gestion de l
adolescence. Elles cibleront aussi bien les jeunes que leurs parents, les leaders d
opinion et les d
cideurs politiques. La mise en
uvre se fera
travers l
organisation des s
ances de causeries
ducatives, des pr
ches, des caravanes, des journ
es de plaidoyer, la diffusion des spots radio t
s, des sketchs, la tenue de th
tre forum. Les capacit
s techniques et mat
rielles des acteurs seront renforc
travers des sessions de formation et ou des recyclages et la production des supports
ducatifs. La strat
gie de la pair-
ducation sera privil
e pour atteindre les cibles.
The
Planification familiale au Niger : plan d
action, 2012-2020
includes an FP communication intervention that targets multiple stakeholder groups, including youth, but does not provide details regarding the purpose of the communication materials or activities within the intervention:
Renforcer la communication
travers le marketing social et le partenariat avec les leaders religieux et traditionnels, les
lus locaux, les ONG [organisations non gouvernementales] et associations, les groupements f
minins et les jeunes chaque ann
e dans les huit r
gions du pays.
The
Planification familiale au Niger: plan op
rationnel, 2018
includes a demand-generation objective to increase the number of opinion leaders and champions in support of FP:
Objectif CD 1 : Augmenter le nombre de leaders d'opinion Champions de la PF
D
finition de l
Objectif : Les leaders d'opinion sont des mod
les pour la soci
. Ils pourront contribuer
la promotion de la PF en parlant publiquement de ses b
fices pour le bien-
tre des communaut
s. Le MSP [minist
re de la Sant
publique] va identifier plus de leaders d'opinion afin qu'ils soutiennent activement et plaident pour les programmes de PF. Il va former les leaders et les outiller avec des donn
es probantes sur la valeur de la PF pour en faire des Champions.
Action Prioritaire
: Identifier et former en plaidoyer et IEC/CCC [information-
ducation-communication /communication pour le changement de comportement] des champions PF au niveau des institutions, religieux, soci
s civiles, secteurs priv
s, jeunes
However, while both the objective and priority action
suggest an intention to increase community support for FP services, it is not evident that the focus is on increasing community support for youth access to FP services in particular.
The
Plan de d
veloppement sanitaire, 2017-2021
describes awareness-raising activities as an intervention to improve the health of young children and adolescents:
Les interventions suivantes seront mises en
uvre pour am
liorer la sant
du jeune enfant et de l
adolescent :
- Pr
venir les grossesses pr
coces chez les adolescentes. Cette intervention sera men
e en collaboration avec le Minist
re en charge de la population, de l
enseignement secondaire, de la jeunesse, de l
emploi et de la justice. Elle consistera
la sensibilisation de la communaut
, les parents et les adolescents afin de r
duire les mariages pr
coces.
- Etendre les activit
s des pairs
ducateurs. Les exp
riences r
ussies des pairs
ducateurs vont
tre
tendues.
- D
autres interventions se feront en amont en termes de communication pour le changement des comportements
la fois des jeunes et des parents. Ces interventions auront pour but d
amener les jeunes
adopter un comportement sexuel responsable et
utiliser les services de sant
disponibles le cas
ant. Ces interventions n
cessitent une action multisectorielle qui implique les m
dias, la soci
civile et la communaut
.
While all reviewed action and operational plans include activities to sensitize communities around youth sexual and reproductive health, prevent teenage pregnancies, and create FP champions in the community,
it is unclear whether the intention is to increase demand for FP or to build a supportive environment for youth FP.
The
Politique nationale de genre, 2017
acknowledges the need for Niger to put more emphasis on policies that encourage the use of family planning to reach true gender equality, and includes a strategic goal that specifically mentions reproductive health:
Axe strat
gique 1 : Am
lioration de l
environnement socioculturel en lien avec la d
mographie, la paix et la s
curit
pour plus d
quit
entre les hommes et les femmes.
Cet axe concerne les changements de mentalit
s des hommes et des femmes, les attitudes et les pratiques propices
galit
de reconnaissance et de traitement envers les femmes y compris le renforcement de leurs capacit
s de d
cision et d
action. Il soutient l
s des femmes aux services sociaux de base (Sant
, Sant
de la Reproduction, Education, Citoyennet
Responsable, Eau, Hygi
ne et Assainissement, etc.) qui sont d
terminants dans la constitution des capacit
s et du capital humain du pays.
The goal details a list of actions to take, including promoting a sociocultural environment favorable to equity; ensuring the different reproductive health needs of women, adolescents, and men; and promoting the participation of women and young people. These activities will be carried out through a program of social mobilization and advocacy of various actors in society to reach gender equity and equality at the household and community levels.
While the policy does identify traditional chiefs and religious leaders as strategic actors who should support awareness raising and social mobilization for the desired structural changes in gender equity, no activities specifically address gender norms within youth FP.
In the absence of this information explicitly addressing efforts to build community support for FP for youth, the country is placed in the gray category, subject to updating if further policy documents provide additional information regarding the content of this intervention.
The
National Standards & Minimum Service Package for Adolescent & Youth-Friendly Health Services, 2018
protects the confidentiality of information for youth and adolescents, including from parents.
The
National Adolescent & Youth Friendly Job Aids for Service Providers in Primary Health Care Facilities in Nigeria, 2015
directs providers to allow youth and adolescents to decide how much they would like to involve their parents in their health care, and to not share any information with parents unless entrusted to by the client.
Although not yet passed, a draft version of the
National Policy on the Health and Development of Adolescents and Young People in Nigeria, 2020-2024
guarantees access to FP services without the consent of a third party:
Ensure that all adolescents age 14 years have the rights to receive ambulatory and non-surgical reproductive health services appropriate for their age and health situation
including contraceptive information, counselling and services, prevention and treatment of sexually transmitted infections, management of sexual abuse and post-abortion care
without any discrimination from health worker or request for adult/parental
consent that may pose a barrier to prompt and quality services
While some policies of Nigeria protect confidentiality of information from parents, none of the policies or enacted laws explicitly affirm youth access to FP services without parental consent. Furthermore, there is no language in Nigerian laws or policies guaranteeing youth access to FP services without consent from spouses or partners. The ambivalence of the current legal framework on youth
s right to freely and independently access FP services creates a barrier for youth accessing such services. Nigeria is placed in the gray category for this indicator. If the National Policy
or another policy with similar language
becomes law, Nigeria
s policy environment would be supportive of youth access to FP services without parental or spousal consent.
The
National Standards & Minimum Service Package for Adolescent & Youth-Friendly Health Services, 2018
promote the right of young people to access general health services without provider discrimination:
Standard 4:
All young people who visit health service delivery facilities are treated with respect, dignity and in an equitable manner irrespective of their health, socio-demographic or political status.
What does this mean? Health care providers administer the same level of quality care and consideration to all adolescents regardless of age, sex, social status, cultural background, ethnic origin, sexual preferences, disability or any other reason.
Rationale: Being treated disrespectfully is a strong disincentive for adolescents and other young people to use health services. Also, young people are not likely to attend a point of service delivery if they feel excluded or discriminated against in any way. On the other hand, being treated equally will have a positive effect on adolescents, encouraging them to meet further appointments and recommend the service to their peers. Furthermore, the manner young people are treated contributes significantly to their sense of satisfaction with care as clients.
Input Criteria:
Protocols/ guidelines to provide services competently in nonjudgmental, caring, considerate, gender-responsive and culturally sensitive attitude and equitable manner are in place.
While the National Standards underscore health providers
obligation to serve youth without discrimination, they do not explicitly mention FP services or identify FP as part of the package of services. A draft version of the
National Policy on the Health and Development of Adolescents and Young People in Nigeria, 2020-2024
states that adolescents older than age 14 should be able to receive contraceptive services without discrimination from a health worker:
Ensure that all adolescents age 14 years have the rights to receive ambulatory and non-surgical reproductive health services appropriate for their age and health situation
including contraceptive information, counselling and services, prevention and treatment of sexually transmitted infections, management of sexual abuse and post-abortion care
without any discrimination from health worker or request for adult/parental
consent that may pose a barrier to prompt and quality services.
If this draft policy is passed with the current language, Nigeria
s policies would acknowledge providers
duty to offer FP services to youth without discrimination or bias. However, Nigeria is currently placed in the gray category for this indicator.
Several key policies acknowledge clients
rights to access sexual and reproductive health services regardless of age. The
National Reproductive Health Policy, 2017
states:
All Nigerians, irrespective of their gender and age including adolescents from age 10 years and older population, have sexual and reproductive rights, and are equally entitled to sexual and reproductive health development and care.
The
National Family Planning/Reproductive Health Service Protocols, Revised Edition, 2010
direct service providers to inform every client of his or her right to:
Access
obtain services regardless of age, sex, creed, colour, marital status, or location.
The
National Youth Policy, 2019
confirms the right of youth to access reproductive health services and alters the definition of youth from the previous youth policy from ages 18 to 35 to ages 15 to 29.
This recognition of the rights of all people to access FP services is critical to addressing the barriers women of all ages frequently face when attempting to access contraception. Nigeria is placed in the green category for this indicator.
The
National Family Planning/Reproductive Health Service Protocols, Revised Edition, 2010
direct service providers to inform every client of their right to:
Access
obtain services regardless of age, sex, creed, colour, marital status, or location.
Nigeria is placed in the green category for this indicator.
The
National Training Manual for the Health and Development of Adolescent and Young People in Nigeria, 2011
discourages providers from recommending certain nonpermanent contraceptive method options, even though they have been deemed safe for general use by the World Health Organization (WHO):
Other methods of contraception are available, but they are often not recommended for youths who have never had children. These methods include Intra-Uterine Devices (IUD), Injectables (Depo-Provera and Noristerat), Tubal ligation, Vasectomy.
The same document further lists three methods deemed most appropriate for youth in the instructions for providers on contraceptive method counseling:
Present a brief lecture covering the three methods of contraception, which are most appropriate for young people
pills, condoms and spermicide e.g. foaming tablets.
The
National Guidelines for the Integration of Adolescent and Youth Friendly Services into Primary Health Care Facilities in Nigeria, 2013
include specific directives to provide contraceptive counseling and services as a part of all clinical preventive services targeting adolescents and youth in primary health care facilities. The list of essential drugs, however, limits contraceptive offerings to barrier methods, oral contraceptives, and emergency contraception. While an intrauterine device (IUD) kit is listed in the medical equipment addendum, this contraceptive offering is absent in the essential drug list.
Providers are discouraged from providing long-acting reversible contraceptives (LARCs) to youth under these policies. The
National Adolescent & Youth Friendly Job Aids for Service Providers in Primary Health Care Facilities in Nigeria, 2015
reaffirm language from previous policies that restricts method mix for young people:
Not all the modern methods of contraceptives are appropriate for adolescents. Most of the temporary methods are appropriate but not the permanent methods.
Furthermore, a national strategy to increase access to LARCs,
Increasing Access to Long-Acting Reversible Contraceptives in Nigeria: National Strategy and Implementation Plan, 2013-2015,
does not include a targeted strategy to increase uptake of LARCs among youth.
However, an earlier document,
National Family Planning/Reproductive Health Service Protocols, Revised Edition, 2010,
includes youth and nulliparous women in the eligibility criteria for short-acting and long-acting reversible contraceptive methods. The document outlines no restrictions on the provision of oral contraceptives and implants to women between menarche and 18 years old and advises providers that the advantages outweigh the risks for the provision of injectables and IUDs to women who are younger than age 18 and nulliparous. The
National Training Manual on Peer-to-Peer Youth Health Education, 2013
also acknowledges that, except for permanent methods, all methods appropriate for healthy adults are also appropriate for post-pubertal adolescents. In addition, the
National Standards & Minimum Service Package for Adolescent & Youth-Friendly Health Services, 2018
specify that the package of adolescent and youth-friendly services for sexual and reproductive health include counseling and provision of barrier methods, oral pills, emergency contraception, and LARCs as
appropriate.
The
Manual for Training Doctors and Nurse/Midwives on LARC Methods, 2015
mandates that providers use the WHO medical eligibility criteria in the provision of IUDs and contraceptive implants but does not reference age.
The inconsistency between the adolescent policies and general FP service protocols creates an opportunity for providers to differentially interpret the directives and a barrier to youth attempting to access a full range of methods. Adding a provision that explicitly supports youth access to all medically eligible contraceptive methods would strengthen Nigeria
s policies regarding youth FP and support full implementation of the
Nigeria Family Planning Blueprint, 2020-2024,
which acknowledges this ambiguity and promotes the provision of LARCs. Nigeria is placed in the red category for this indicator.
Although the availability of emergency contraception (EC) is not factored into the categorization of this indicator, the
National Family Planning/Reproductive Health Service Protocols, Revised Edition, 2010,
the
Clinical Protocol for the Health and Development of Adolescent and Young People in Nigeria, 2011
and the
National Adolescent & Youth Friendly Job Aids for Service Providers in Primary Health Care Facilities in Nigeria, 2015
all include EC as a possible contraceptive method for youth.
Nigeria
s policy environment surrounding sexuality education is weak. The leading guidance on provision of sexuality education in the country is the
National Family Life and HIV Education Curriculum for Junior Secondary School in Nigeria, 2003.
This document provides a substantial overview of the family life and HIV education (FLHE) curriculum for junior secondary schools, primarily focused on human development and life skills. The component of the curriculum most relevant to contraceptive provision is HIV education. While the curriculum presents comprehensive information on sexually transmitted infections (STI)/HIV, including definitions, modes of transmission, and signs and symptoms, it falls short of informing youth on how to prevent these infections through safe sexual behavior and condom and contraceptive use. Further, there is no discussion of where or how to access sexual and reproductive health services. Rather, the guidance for preventing STI/HIV is:
- Abstain from sexual behavior.
- Avoid sharing sharp objects (such as needles, razor, clippers).
- Insist on screened blood.
The
National Guidelines on Promoting Access of Young People to Adolescent and Youth-Friendly Services in Primary Health Care Facilities in Nigeria, 2013
references peer education as a strategy to supplement in-school instruction on sexual and reproductive health to reach in-school and out-of-school youth, as well as parents and guardians. The
National Training Manual on Peer-to-Peer Youth Health Education, 2013
details a peer education session on contraception and pregnancy prevention, including a discussion emphasizing the benefits of abstinence. However, the policy also states that peer educators should discuss various contraceptives and their advantages, acknowledging that
adolescents should make contraceptive choices based on their need and whether they want to protect against pregnancy and or need to protect against STI/HIV.
The
Nigeria Family Planning Blueprint, 2020-2024
outlines the strengthening of nationwide implementation of the FLHE curriculum and increased access to online learning materials.
Although not yet passed, a draft version of the
National Policy on the Health and Development of Adolescents and Young People in Nigeria, 2020-2024
notes the role the Ministry of Education plays in policy implementation, and that the Ministry must review and revise the FLHE curriculum to ensure it conforms to global best practices in CSE curriculum design and delivery.
Moreover, the
National Family Planning Communication Plan, 2017-2020" states that the
National Family Life and HIV Education Curriculum for Junior Secondary School in Nigeria, 2003
will be reviewed and amended
to support the goal of disseminating appropriate FP messaging to adolescents and young people.
It seeks to incorporate FP into classroom settings by disseminating information through peer educators and trained teachers. While this indicates positive language for CSE, the curriculum has yet to be amended and the current policy environment still promotes abstinence
Nigeria is placed in the red category for comprehensive sexuality education (CSE) since the country
s guidance on sexuality education refers only to abstinence. To improve the policy environment surrounding sexuality education, policymakers in Nigeria should consider including the nine United Nations Population Fund (UNFPA) essential components of CSE when updating the FLHE curriculum.
Nigeria
National Reproductive Health Policy, 2017
emphasizes youth-friendly service provision, although such services are not defined:
Objective 4: To increase access to quality reproductive health information and services for adolescents and young persons. Target 1: Achieve at least 50% coverage of young people who have access to comprehensive SRH [sexual and reproductive health] information and services by 2021. Target 2: Achieve at least 50% coverage of young people who have access to comprehensive youth friendly health services by 2021.
The
Nigeria Family Planning Blueprint, 2020-2024
outlines plans to develop a national FP training plan for providers to address bias and ensure nondiscriminatory care, with a specific emphasis on a rights-based approach for youth:
SD.5. Expand access to Rights based Youth Friendly FP Services.
Provider bias in service provision to youth and sexually active unmarried women remains a barrier to the delivery of a right based non-discriminatory FP services. Service provider bias as a result of training being more skill focused with inadequate emphasis on value clarification and youth-friendly services is an identified challenge in service delivery. The Quality of counselling and attitudinal skill-building will be improved by revising FP training materials/curriculum to emphasize right-based approach. IPCC [interpersonal communication and counselling] modules will be made mandatory as a component of FP trainings to ensure it is reinforced as a way of addressing provider attitude and bias as well as institutionalizing rights-based counselling.
A previous version of the Blueprint specifically identified steps to ensure privacy in youth-friendly service delivery spaces. However, while the current Blueprint notes that the national FP training plan
s rights-based approach should be based on confidentiality, it does not specifically address privacy in the provision of youth-friendly FP services.
The
National Youth Policy, 2019
outlines policy benchmarks to integrate adolescent and youth-friendly health services in primary health facilities and implement training programs for youth-friendly service delivery. The
National Training Manual for the Health and Development of Adolescent and Young People in Nigeria, 2011
lists eight competencies of a youth-centered counselor, one of which guides counselors to be aware of their own judgments:
Self awareness and self-knowledge: Develop a keen knowledge and awareness of self in terms of one
s own limitations, biases, prejudices religious and cultural beliefs and internal conflicts.
However, the same document emphasizes abstinence-only values, likely affirming some providers
preconceived notions regarding youth
s right to access contraception. One section describing factors affecting adolescent development mentions abstinence as a positive traditional practice, and a later section describing pregnancy prevention methods emphasizes abstinence as the norm:
Sexual abstinence is the surest way of preventing STIs [sexually transmitted infections] and unwanted pregnancies. In our society where the norm is sexual abstinence, young people practicing
abstinence are free of guilt of being found to have violated the norm, and fear of the consequences of sexual intercourse. Sexual abstinence could also add to the sense of self-esteem and self-worth.
The
National Standards & Minimum Service Package for Adolescent & Youth-Friendly Health Services, 2018
state that provider protocols and guidelines include nonjudgmental services and notes that young people should receive services for free or at a subsidized rate, but is not specific to family planning:
- Protocols/ guidelines to provide services competently in nonjudgmental, caring, considerate, gender-responsive and culturally sensitive attitude and equitable manner are in place.
- All staff undergo training in appropriate procedures to ensure respectful attitude and maintenance of the dignity of clients in their service provision to all categories of young people.
- Policies and procedures to provide health services to young people free of charge or at affordable prices are in place.
Multiple external documents report the existence of Nigeria
Free Family Planning Commodity Policy, 2011,
which states that family planning commodities should be provided free of charge to all clients in the public sector. However, a copy of this policy could not be obtained, and stakeholders note that out-of-pocket costs often offset the policy
s effectiveness.
Nigeria is placed in the yellow category for youth-friendly FP service provision. The country has the potential to move to a green categorization if policy documents include provisions to offer free or subsidized FP services to youth and further clarify steps to ensure audio/visual privacy in services.
The
National Policy on Health and Development of Adolescents and Young People in Nigeria, 2007
briefly addresses the sexual and reproductive health needs of young people. The policy acknowledges that youth face sociocultural barriers to access sexual and reproductive health services:
Negative perception about adolescent sexual and reproductive health issues and related services.
To address these barriers, the policy includes activities to link service delivery with community sensitization efforts targeting parents and mass media activities to shift social norms.
The
National Strategic Framework on the Health and Development of Adolescents and Young People in Nigeria, 2007-2011
includes two relevant objectives:
Promote awareness of reproductive health issues of young people amongst all stakeholders.
Strengthen the capacity of parents, guardians and significant others to respond positively to the needs of young people through effective IEC [information, education, and communication] approaches.
Specific activities are outlined under these objectives to engage the community through advocacy and community mobilization and promote reproductive health behaviors through information, education, and communication. The
National Family Planning Communication Plan, 2017-2020"includes plans to increase engagement of traditional and religious leaders on family planning, which may contribute further to an enabling social environment. The Communication Plan also states that campaigns will use multi-media approaches to reach the general public and specific demand generation efforts would be made for adolescents, youth and other high priority groups.
A draft copy of the
National Adolescent Health Policy, 2020-2024
declares gender equity and responsiveness as an underlying principle and value and emphasizes the need to engage gender-responsive approaches, including community interventions that address gender imbalances:
Strengthen adolescent leadership and engagement in the family and community using transformative interventions that address the power imbalance between adolescent girls and boys as well as gender-inequitable norms and practices, including gender-based violence.
Existing policies, however, do not include specific activities to address gender norms related to youth access to or use of FP services. Nigeria is placed in the yellow category for this indicator.
The
Responsible Parenthood and Reproductive Health Act of 2012, Republic Act 10354
restricts access to FP services for minors:
That minors will not be allowed access to modern methods of family planning without written consent from their parents or guardian/s except when the minor is already a parent or has had a miscarriage.
The Act continues to note that providers may waive parental consent or spousal consent in specific cases:
Section 23. Prohibited Acts.
The following acts are prohibited:
- Any health care service provider, whether public or private, who shall:
.
(2) Refuse to perform legal and medically-safe reproductive health procedures on any person of legal age on the ground of lack of consent or authorization of the following persons in the following instances:
(i)Spousal consent in case of married persons: Provided, that in the case of disagreement the decision of the one undergoing the procedure shall prevail;
(ii) Parental consent or that of the person exercising parental authority in the case of abused minors, where the parent or the person exercising parental authority is the respondent, accused or convicted perpetrator as certified by the proper prosecutorial office of the court. In the case of minors, the written consent of parents or legal guardian or, in their absence, persons exercising parental authority or next-of-kin shall be required only in elective surgical procedures and in no case shall consent be required in emergency or serious cases as defined in Republic Act No. 8344
Section 4.07 of the
Implementing Rules and Regulations of Republic Act No. 10354, 2013
provides more details on the requirement of written consent from a parent or guardian for minors to access family planning services:
Any minor who consults at health care facilities shall be given age-appropriate counseling on responsible parenthood and reproductive health. Health care facilities shall dispense health products and perform procedures for family planning:
Provided, that in public health facilities, any of the following conditions are met:
(a) The minor presents written consent from a parent or guardian.
(b) The minor has had a previous pregnancy or is already a parent as proven by any one of the following circumstances, among others:
- Written documentation from a skilled health professional;
- Documentation through ancillary examinations such as ultrasound;
- Written manifestation from a guardian, local social welfare and development officer, local government official or local health volunteer; or
- Accompanied personally by a parent, grandparent, or guardian.
While the policy environment does not require spousal consent, the Philippines is placed in the red category for this indicator as the law requires parental consent for minors to access FP services.
The
Responsible Parenthood and Reproductive Health Act of 2012, Republic Act 10354
prohibits providers from refusing health care services and information on account of a person
s marital status, gender, age, religious convictions, personal circumstances, or nature of work. However, the act includes language that allows providers to object to services based on their religious beliefs as long as they refer the patient to another provider:
Section 23. Prohibited Acts.
The following acts are prohibited:
(a) Any health care service provider, whether public or private, who shall:
(3) Refuse to extend quality health care services and information on account of the person
s marital status, gender, age, religious convictions, personal circumstances, or nature of work: Provided, That the conscientious objection of a health care service provider based on his/her ethical or religious beliefs shall be respected; however, the conscientious objector shall immediately refer the person seeking such care and services to another health care service provider within the same facility or one which is conveniently accessible: Provided, further, That the person is not in an emergency condition or serious case as defined in Republic Act No. 8344, which penalizes the refusal of hospitals and medical clinics to administer appropriate initial medical treatment and support in emergency and serious cases;
Nevertheless, the
Family Planning Competency-Based Training, Facilitator
s Guide, n.d." and "Family Planning Competency-Based Training, Basic Course Handbook for Service Providers n.d." teach providers to use the World Health Organization (WHO) medical eligibility criteria for contraceptive use and train counselors to not impose their own values on clients, although the latter training is not specific to youth FP.
Since the laws and policies of the Philippines support the WHO medical eligibility criteria for contraceptive use but do not explicitly require providers to service youth despite personal beliefs, the country is placed in the yellow category for this indicator.
The
Family Planning Competency-Based Training, Basic Course Handbook for Service Providers, n.d
lists key policy statements that guide FP program promotion and implementation, one of which includes the provision of FP services based on voluntary and informed choice for all women and men of reproductive age regardless of age:
FP information and services will be provided based on voluntary and informed choice for all women and men of reproductive age regardless of age, number of children, marital status, religious beliefs, and cultural values.
The
Responsible Parenthood and Reproductive Health Act of 2012, Republic Act 10354
also prohibits providers from refusing to offer quality health care services based on age:
Section 23. Prohibited Acts.
The following acts are prohibited:
(a) Any health care service provider, whether public or private, who shall:
.
(3) Refuse to extend quality health care services and information on account of the person
s marital status, gender, age, religious convictions, personal circumstances, or nature of work:
The Philippines is therefore placed in the green category for this indicator.
The
Family Planning Competency-Based Training, Basic Course Handbook for Service Providers, n.d.
includes key policy statements that guide FP program promotion and implementation, one of which includes the provision of FP services for all women of reproductive age regardless of marital status:
FP information and services will be provided based on voluntary and informed choice for all women and men of reproductive age regardless of age, number of children, marital status, religious beliefs, and cultural values.
Moreover, the
Responsible Parenthood and Reproductive Health Act of 2012, Republic Act 10354
prohibits a health care service provider from refusing to provide quality health care services and information because of the person
s marital status, gender, age, religious convictions, personal circumstances, or nature of work.
The Philippines is therefore placed in the green category for this indicator.
According to the
Family Planning Competency-Based Training, Facilitator
s Guide, n.d.
and the
Family Planning Competency-Based Training, Basic Course Handbook for Service Providers, n.d.
all contraceptives are safe for use of young people,
but the documents provide additional notes on the benefits of specific methods:
ALL CONTRACEPTIVES ARE SAFE FOR USE OF YOUNG PEOPLE
Generally, all adolescents are advised to practice ABSTINENCE until they reach the proper age to start a family.
- Fertility awareness-based methods For those adolescents who can effectively monitor body changes to determine the woman
s fertile period and able to follow the rules as to when to abstain from sex. If not able, consider other FP methods.
- Oral contraceptives Low dose COC [combined oral contraceptives]
is a good choice because of high efficacy and low frequency of side effects. Emphasis is needed for consistent and proper use of the methods during counseling along with COC side effects.
- Male condoms One main advantage is its safety. Since they are readily available and accessible in different places and set up. Education and counseling are important to ensure correct and consistent condom use.
- Progestin-only injectables For those adolescents having difficulty in using COCs, progestin-only injectables are suitable alternatives.
- IUD Not a good choice for young women who are at high risk for STIs [sexually transmitted infections]. IUD [intrauterine devices] can be an option for parous adolescents who require long-term protection against pregnancy and have a low risk of STIs.
Moreover, "The Philippine Clinical Standards Manual on Family Planning, 2014
states that "all currently available modern contraceptive methods are safe for adolescents" and provides descriptions of each method
including combined hormonal contraceptives, progesterone-only contraceptives, barrier methods, IUDs, fertility-based methods, and sterilization
along with recommended reasons for use/avoidance.
Furthermore, the "Adolescent Health and Development Program: Manual of Operations 2017" requires local governments to provide basic adolescent health care services, including the purchase and distribution of family planning commodities:
LGUs [local government units] must ensure provision of basic adolescent health care services including, but not limited to, the operation and maintenance of facilities and equipment necessary for the delivery of a full range of reproductive health care services and the purchase and distribution of family planning goods and supplies as part of the essential information and service delivery package defined by DOH [Department of Health].
While the Basic Course Handbook for Service Providers does not address youth access to a full range of methods, it does state that men and women should access methods of their choice:
FP information and services will be provided based on voluntary and informed choice for all women and men of reproductive age regardless of age, number of children, marital status, religious beliefs, and cultural values.
While Filipino policies identify FP methods available to youth and acknowledge youth access to all contraceptives, they do not sufficiently state that youth have access to a full range of methods, including long-acting reversible contraceptives (LARCs), regardless of age, marital status, or parity. The Philippines is placed in the yellow category for this indicator.
The
National Policy and Strategic Framework on Adolescent Health and Development, Administrative Order No. 2013-0013
tasks the Departments of Health, Education, and Social Welfare and Development with formulating
an age- and development-appropriate Reproductive Health and Sexuality Education curriculum.
Similarly,
The Responsible Parenthood and Reproductive Health Act of 2012, Republic Act 10354
outlines the government
s plan for age-appropriate reproductive health education:
Section 14. Age- and Development-Appropriate Reproductive Health Education.
The State shall provide age- and development-appropriate reproductive health education to adolescents which shall be taught by adequately trained teachers informal and nonformal educational system and integrated in relevant subjects such as, but not limited to, values formation; knowledge and skills in self-protection against discrimination; sexual abuse and violence against women and children and other forms of gender based violence and teen pregnancy; physical, social and emotional changes in adolescents; women
s rights and children
s rights; responsible teenage behavior; gender and development; and responsible parenthood:
Provided, That flexibility in the formulation and adoption of appropriate course content, scope and methodology in each educational level or group shall be allowed only after consultations with parents-teachers community associations, school officials and other interest groups. The Department of Education (DepED) shall formulate a curriculum which shall be used by public schools and may be adopted by private schools.
Furthermore,
Implementing Rules and Regulations of the Responsible Parenthood and Reproductive Health Act of 2012
states that private and public schools shall provide a supportive environment for youth wherein they have access to facilities for information and referral to service providers on all responsible parenthood and reproductive health concerns. The act also notes that reproductive health information provided to youth should be scientifically accurate and evidence-based information on the reproductive system.
The
Adolescent Health and Development Program: Manual of Operations, 2017
refers to a comprehensive sexuality education (CSE) activity called
Abstinence-Plus,
which focuses on abstinence as the best method to avoid an unintended pregnancy and contraception as a way to reduce risk. The Manual of Operations further states that the content of its curriculum:
- Created safe social environment for youth participants
...
- Focused narrowly on specific sexual behaviors that lead to these health goals (e.g., abstaining from sex, using condoms); gave clear messages about these behaviors; addressed how to avoid situations that might lead to these behaviors
- Used teaching methods that actively involved youth participants and helped them to personalize the information.
- Made use of activities appropriate to the young people
s culture, developmental level, and previous sexual experience.
While existing Filipino laws and guidelines support the provision of sexuality and reproductive health education, they do not specifically address education in the context of education for family planning. The Philippines is placed in the yellow category for this indicator and can improve by referencing the UNFPA essential components of CSE in future curricula.
The Philippine Clinical Standards Manual on Family Planning, 2014
states that young individuals must be assured confidentiality and privacy and that reproductive health counseling services for them must be made accessible, available, affordable, and understandable in a supportive and non-judgmental environment.
The Responsible Parenthood and Reproductive Health Act of 2012, Republic Act 10354
states that the government should guarantee affordable reproductive health services, methods, devices, and supplies to all clients. The Act notes that individuals targeted in the National Household Targeting System for Poverty Reduction shall be beneficiaries to free reproductive health services and supplies but does not specifically address youth.
The
Family Planning Competency-Based Training: Basic Course Handbook for Service Providers, n.d.
includes key policy statements that guide FP program promotion and implementation, one of which states that privacy and confidentiality should always be observed while providing services.
The
Implementing Rules and Regulations of the Responsible Parenthood and Reproductive Health Act of 2012
instructs the Department of Health to develop a curriculum to train health professionals in counseling about adolescent reproductive health, determining age- and development-appropriate methods or services.
In addition, the
Adolescent Health and Development Program: Manual of Operations 2017
which is designed to provide recommendations and tools for health care facilities
includes a section on enhancing providers
capacity and notes that changing providers
attitudes, beliefs, knowledge, and practices should be carried out through sensitization and training. The document notes that sensitization should be used to persuade health professionals to view adolescent health as a public health and human rights problem and training should be used to improve providers
knowledge and skills on adolescent-friendly services. The Manual also lays out levels of compliance to standards, which detail that health facilities should ensure audio/visual privacy in facilities and implement procedures to ensure privacy and confidentiality.
The
Adolescent Job Aid Manual, 2009
directs facility staff to
ensure that the consultation and examination are done in a place where the interaction between the health worker and the adolescent cannot be heard or seen by anyone else.
However, the manual outlines general standards for all adolescent health services and is not specific to youth FP.
While Filipino laws and policies refer to youth access to FP services, core elements youth-friendly service delivery are not explicitly detailed, such as trainings to offer non-judgmental services to adolescents and affordability in the context of FP services for youth. The Philippines is placed in the yellow category for this indicator.
The
National Policy and Strategic Framework on Adolescent Health and Development, Administrative Order No. 2013-0013
tasks the Department of Health, Department of Education, and the Department of Social Welfare and Development to:
Provide parents with adequate and relevant scientific materials on the age- appropriate topics and manner of teaching Reproductive Health and Sexuality Education to their children.
The "Responsible Parenthood and Reproductive Health Act of 2012, Republic Act 10354
directs the Department of Health and local government units to initiate and sustain a heightened nationwide multimedia campaign to raise public awareness on the protection and promotion of family planning and youth reproductive health, among other issues. It also acknowledges the role gender equity should play in the government
s reproductive health efforts:
Moreover, the State recognizes and guarantees the promotion of gender equality, gender equity, women empowerment and dignity as a health and human rights concern and as a social responsibility. The advancement and protection of women
s human rights shall be central to the efforts of the State to address reproductive health care.
While not specific to youth family planning, the National Standards for Adolescent-Friendly Services outlined in the
Adolescent Health and Development Program: Manual of Operations, 2017
include a standard to create an enabling environment:
An enabling environment exists in the community for adolescents to seek and utilize the health services that they need...
The related input criteria include procedures to communicate with adults visiting the health facility about the value of providing adolescents with services and activities
including community assemblies, meetings with parents, group meetings, and school visits
to engage community members in providing adolescent health services.
While
The Philippine Youth Development Plan, 2017-2022,
includes plans to implement
Responsible Parenthood and Family Planning classes
and increase subscription to family planning for the youth, it does not provide any detailed strategy.
The Philippines
legal and policy environment is promising as it outlines plans to raise public awareness on youth access to sexual and reproductive health services. However, provisions of most policies do not have an explicit focus on FP services for youth. While the Youth Development Plan states specific plans to improve family planning for youth, it does not provide any details on the nature of classes or interventions for making family planning information available. Other policies also use vague language about building community support or addressing gender and social norms without identifying specific activities or interventions.
The Philippines is placed in the gray category for this indicator.
The policy documents reviewed for Senegal contain no references to parental or spousal consent. Senegal is placed in the gray category for this indicator.
The
Plan strat
gique de sant
sexuelle et de la reproduction des adolescent(e)s/jeunes au S
gal, 2014-2018
states that services must be provided to youth by providers who are nonjudgmental:
Ces services doivent
tre :
...
efficaces : ils sont assur
s par des prestataires disponibles, comp
tents, accueillants qui savent communiquer avec les jeunes sans porter de jugement de valeur.
Therefore, Senegal is placed in the green category for this indicator.
The right of youth to receive sexual and reproductive health care is written into Senegalese law. The 2005 reproductive health (RH) law,
Loi n
2005-18 du 5 ao
t 2005 relative
la sant
de la reproduction,
includes a clear declaration allowing all people to access RH services without discrimination, including discrimination based on age. Under Articles 3 and 10, the right to RH is acknowledged as a fundamental health and human right for all people. The law further promotes access to RH for adolescents under Article 4:
Article 3 : Le droit
la Sant
de la Reproduction est un droit fondamental et universel garanti
tout
tre humain sans discrimination fond
e sur l
ge, le sexe, la fortune, la religion, la race, l
ethnie, la situation matrimoniale ou sur toute autre situation.
Article 4 : Les Soins et services de Sant
de la Reproduction recouvrent :
la promotion de la sant
de la reproduction des adolescents ;
Article 10
: Toute personne est en droit de recevoir tous les soins de sant
de la reproduction sans discrimination fond
e sur l
ge, le sexe, le statut matrimonial, l
appartenance
un groupe ethnique ou religieux.
Senegal is placed in the green category for this indicator since national laws and policy guidelines support adolescents
access to contraception regardless of age.
The
Loi n
2005-18 du 5 ao
t 2005 relative
la sant
de la reproduction
includes a clear declaration allowing all people to access reproductive health services without discrimination, including discrimination based on marital status:
Article 3 : Le droit
la Sant
de la Reproduction est un droit fondamental et universel garanti
tout
tre humain sans discrimination fond
e sur l
ge, le sexe, la fortune, la religion, la race, l
thnie, la situation matrimoniale ou sur toute autre situation.
Article 4 : Les Soins et services de Sant
de la Reproduction recouvrent:
la promotion de la sant
de la reproduction des adolescents;
Article 10. - Toute personne est en droit de recevoir tous les soins de sant
de la reproduction sans discrimination fond
e sur l
ge, le sexe, le statut matrimonial, l
appartenance
un groupe ethnique ou religieux.
Because the law includes FP as a part of reproductive health care and services, Senegal is placed in the green category for this indicator.
The right to a full range of contraceptive options is explicitly outlined in the
Protocoles de services de sant
de la reproduction au S
gal, n.d.
The Protocoles de services recognize the unique sexual and reproductive health needs and interests of youth and instruct providers to offer medically appropriate contraception to adolescents, regardless of age:
En ce qui concerne la planification familiale, les adolescents peuvent utiliser n
importe quelle m
thode de contraception et doivent avoir acc
un choix
tendu. L
ge ne constitue pas
lui seul une raison m
dicale permettant de refuser une m
thode
une adolescente. Si certaines inqui
tudes ont
exprim
es concernant l
utilisation de certaines m
thodes contraceptives chez l
adolescente (par ex. l
emploi des progestatifs injectables seuls pour les moins de 18 ans), elles doivent
tre pes
es en regard des avantages pr
sent
s par le fait d
viter une grossesse.
Additionally, the
Protocoles de services
include long-acting reversible contraceptives in the list of available methods. Therefore, Senegal is placed in the green category for this indicator.
Although the availability of emergency contraception is not factored into the categorization of this indicator, emergency contraception is also included in the list of available methods in the
Protocoles de services.
In the early 1990s, two family life education (FLE) programs were piloted in Senegal. In 1990, the Ministry of Education (MoE) piloted a population education curriculum in primary schools. In 1994, the MoE appointed le
Groupe pour l
tude et l
Enseignement de la Population,
a Senegalese nongovernmental organization, to pilot an FLE program in secondary schools. In 2010, the MoE incorporated aspects of the FLE pilot programs into the national basic education curriculum; however, critical elements of comprehensive sexuality education (CSE) were omitted, including
rights, gender, personal values, interpersonal relationships, gender-based violence, skills-building related to sexual and reproductive health (SRH) (for example, negotiating condom use), and critical thinking skills to assess social norms."
The MoE has facilitated efforts to refresh the national curriculum. In doing so, the policy revision should consider the nine United Nations Population Fund (UNFPA) essential components of CSE.
The
Plan strat
gique de sant
sexuelle et de la reproduction des adolescent(e)s/jeunes au S
gal, 2014-2018
describes the aims of a proposed sexual health education program, including some of the essential components of CSE programs. It describes strengthening skills in critical thinking, personalization of information, and reaching across formal and informal sectors and across age groups. For example:
L'
ducation
la sant
sexuelle consiste
informer sur la sexualit
en transmettant un certain nombre de valeurs et de recommandations aux adolescent(e)s/jeunes. En effet elle vise
velopper l'exercice de l'esprit critique, notamment par l'analyse des mod
les et des r
les sociaux v
hicul
s par les m
dias.
Elsewhere, the Plan strat
gique describes educating youth on human rights and gender inequalities:
Dans le cadre de l'
ducation de ces derniers, les questions de genre et les cons
quences n
fastes de la violence bas
e sur le genre seront abord
es afin que toute forme de violence soit pr
venue. Les jeunes seront inform
s et sensibilis
s sur les Droits Humains (le genre faisant partie int
grante des questions de droit de l'homme).
This component, however, is not included as an aim of the previously described sexual health education program. Additional components, such as providing accurate information, linking SRH services and other initiatives for young people, providing youth-friendly spaces, and strengthening youth input into SRH programming, are also acknowledged in the
Plan strat
gique,
but often in the context of service delivery rather than CSE.
The
Cadre strat
gique national de planification familiale, 2016-2020
includes interventions for the promotion of large-scale communication on birth spacing. In reference to communication to young people, the
Cadre strat
gique national
outlines the integration of new family planning protocols into current home economics and life and earth sciences curricula and the support of peer educators within FLE clubs as interventions:
Renforcement de la communication visant les jeunes
:
En mati
re de renforcement de la communication visant les jeunes,
la DSRSE [direction de la sant
de la reproduction et de la survie de l
enfant] mettra l
accent sur des initiatives visant
adapter davantage le dispositif de formation existant en formant les professeurs relais technique (PRT) et les professeurs d'
conomie familiale sur la PF, en appuyant l
gration des nouveaux protocoles PF dans les curricula des professeurs d'
conomie familiale et de Sciences de la Vie et de la Terre en formant les leaders El
ves Animateurs (LEA), les gouvernements scolaires et autres pairs
ducateurs sur les techniques de communication. Enfin, le pr
sent plan pr
voit de r
aliser des investissements substantiels visant
doter les LEA de supports de communication, contractualiser avec les clubs EVF [
ducation
la vie familiale] dans les
coles pour la mise en oeuvre d'un paquet d'activit
s et soutenir la r
alisation d
activit
riodiques de suivi /coordination.
The
Strat
gie nationale de financement de la sant
pour tendre vers la couverture sanitaire universelle, 2017
acknowledges the positive impact that sexual health education can have on informed decisions and reproductive health outcomes, but does not provide further details on the proposed education curriculum.
Senegal
s policies acknowledge CSE broadly but fall short of including all nine essential components together in a clear operational policy for CSE. Senegal has a promising policy environment for CSE, but until these policies are revised, the country will remain in the yellow category for this indicator.
The
Plan strat
gique de sant
sexuelle et de la reproduction des adolescent(e)s/jeunes au S
gal, 2014-2018
includes plans to train providers to offer youth-friendly contraceptive services, with particular emphasis on good communication skills:
Pour le professionnel de sant
, le dialogue et la relation de confiance nou
s avec l'adolescent(e)/ jeune sont des d
terminants fondamentaux de la qualit
de la prise en charge, qu'il s'agisse de diagnostiquer, de d
pister et d'informer. En effet, il doit avoir des comp
tences n
cessaires pour communiquer avec les adolescent(e)s/jeunes, d
tecter leurs probl
mes de sant
de fa
on pr
coce et fournir des conseils et des traitements. Il doit placer les besoins, les probl
mes, les pens
es, les sentiments, les points de vue et les perspectives des adolescent(e)s/jeunes, au c
ur de ses activit
s... L'accent sera mis sur l'apprentissage et la formation continue.
Additionally, the
Plan strat
gique
outlines the necessary criteria for youth-friendly services in line with the World Health Organization Quality of Care framework for adolescent service provision, including that services must be accessible (and affordable), acceptable, equitable, effective (and without any value judgments), appropriate, efficient, and comprehensive:
Ces services doivent
tre :
- accessibles : ils sont disponibles au bon endroit, au bon moment,
un bon prix (gratuit si n
cessaire).
- acceptables : ils r
pondent
leurs attentes et garantissent la confidentialit
.
-
quitables : ils sont offerts
tous sans distinction de sexe, d'
ge, de religion, d'appartenance ethnique, de handicap, de statut social ou de toute autre nature.
- efficaces : ils sont assur
s par des prestataires disponibles, comp
tents, accueillants qui savent communiquer avec les jeunes sans porter de jugement de valeur.
- appropri
s : les soins essentiels sont fournis d'une mani
re id
ale et acceptable dans un environnement s
curis
.
- efficients : les soins de qualit
sont dispens
s au co
t le plus faible possible.
- complets : la prestation de soins couvre tous les aspects de la prise en charge et la r
rence est assur
e en cas de besoin.
The
Plan d
action national de planification familiale, 2012-2015
further references the provision of FP services to youth and identifies the need for discretion, confidentiality, and tailored service provision:
L
accent sera mis sur la qualit
du service et du counseling tout en assurant la disponibilit
du mat
riel et des consommables. Un focus particulier sera mis sur l
lioration de l
s aux services de Planification Familiale pour les jeunes en leur assurant la discr
tion, la confidentialit
et un service adapt
.
Similarly, the
Protocoles de services de sant
de la reproduction au S
gal, n.d.
include a direct reference to the provision of FP services for youth and recognize the rights of youth to receive services, including their right to information, access, privacy, and dignity.
Les protocoles d
finis doivent
tre respect
s pour les diff
rents services. Cependant du fait de la sp
cificit
et de la vuln
rabilit
de cette cible, une attention particuli
re doit
tre apport
e aux droits
information,
intimit
et
la dignit
de ces adolescent(e)s et jeunes.
Across these policies, all three service delivery elements of adolescent-friendly contraceptive service provision are addressed. Therefore, Senegal is placed in the green category for this indicator.
The
Plan d
action national de planification familiale, 2012-2015
highlights the need to inform youth and their communities regarding FP. One of the strategic actions under the communication plan is to roll out a mass media campaign aimed at young people. This strategic action has three main activities:
B
tir une campagne participative pour les jeunes
Renforcer les centres d'
coute pour les jeunes et centres d'informations
Utilisation des r
seaux sociaux et nouvelles technologies pour informer les jeunes sur la PF (facebook, sms, blogs)
The
Plan strat
gique de sant
sexuelle et de la reproduction des adolescent(e)s/jeunes au S
gal, 2014-2018
includes plans to use information and communications technology and media to reach youth and the broader community.
Une campagne nationale m
diatique de sensibilisation sur la SRAJ [sant
reproductive des adolescents et des jeunes] sera
galement men
e. De m
me il serait judicieux d'utiliser des radios communautaires qui repr
sentent un moyen de mobilisation important, pour garantir la participation de la communaut
.
The
Plan strat
gique
also discusses how gender will be addressed in youth reproductive health programs:
6.4.2.1 Sur le plan social et organisationnel
Des actions
mener pour l'am
lioration de l'environnement social/organisationnel sont indispensables pour l'atteinte des objectifs de la SRAJ...
Prise en compte des questions de Genre
La dimension genre sera prise en compte dans l'
laboration des projets et programmes de SRAJ ainsi que dans 1'
ducation et la formation des adolescent(e)s/jeunes. Dans le cadre de l'
ducation de ces derniers, les questions de genre et les cons
quences n
fastes de l
violence bas
e sur le genre seront abord
es afin que toute forme de violence soit pr
venue.
Les jeunes seront inform
s et sensibilis
s sur les Droits Humains (le genre faisant partie int
grante des questions de droit de l'homme).
Since these plans include detailed steps to build an enabling social environment among youth and communities for FP services, Senegal is placed in the green category for this indicator.
The
Reproductive and Healthcare Rights Act, 2013,
a law applicable across Pakistan, signals increased political acknowledgment of the reproductive rights of women, in an effort to curtail maternal mortality and morbidity. While the Act provides increased legal protection for women overall, it ignores the particular reproductive health (RH) rights of young women.
The Act does not include any provision for youth. Further, under Line B, Article 4, the right of parents to educate their children is prioritized as a means of promoting RH care information. The acknowledgment of parental responsibility without subsequent recognition of youth
s rights to FP services creates an opportunity for interpretation that favors parental rights over children
s RH decisions.
Article 4: Promotion of reproductive healthcare rights:
1. The right to reproductive healthcare information can be promoted,...
(b) through the exercise of parental responsibility which assures the right of parents as educators.
The Sindh policies reviewed do not provide further guidance on youth
s right to access FP services without parental consent, leaving ambiguity in the requirement of parental consent for FP services.
The
Manual of National Standards for Family Planning, 2009
and the
Manual of Standards for Family Planning Services, Sindh, Revised, 2017
include identical guidance to providers on preventing barriers to contraceptive use, including the discouragement of requiring spousal consent:
Eligibility requirements that needlessly limit the use of certain methods based
on a woman
s age, parity, or lack of spousal consent.
The national and provincial standards advise providers to follow the World Health Organization
s medical eligibility criteria when offering contraception to women. While the policies address spousal consent, they fail to sufficiently address parental consent for youth to access FP services. Sindh is placed in the yellow category for this indicator.
The
Manual of National Standards for Family Planning, 2009
and the
Manual of Standards for Family Planning Services, Sindh, Revised, 2017
both of which include youth access to FP as part of their standards
identify unjustified medical barriers, including provider bias:
What Are Unjustified Medical Barriers?
- Practices derived (at least partly) from a medical rationale.
- Non-evidence-based barriers that result in denial of contraception.
- Eligibility restrictions, based on providers
limitations/personal biases.
These policies urge providers to follow the medical eligibility criteria to discern eligibility for contraceptive services. Sindh is placed in the green category for this indicator.
The
Costed Implementation Plan on Family Planning for Sindh, 2015
includes
Family Planning 2020: Rights and Empowerment Principles of Family Planning
as an annex. This list states that age and marital status should not determine access to FP services:
Quality, accessibility, and availability of information and services
should not vary by non-medically indicated characteristics i.e. age, location, language, ethnicity,
disability, HIV status, sexual orientation, wealth, marital or other status.
This declaration references the right of all people to access services regardless of age, placing Sindh in the green category for this indicator.
Sindh policy documents are contradictory regarding the right to access FP services regardless of marital status. The
Costed Implementation Plan on Family Planning for Sindh, 2015
references the right of all women, regardless of marital status, to access FP information and services, as does the
Manual of Standards for Family Planning Services, Sindh: Revised, 2017
:
Right to Access: All individuals in the community have a right to receive services from FP programmes, regardless of their social status, economic situation, religion, political belief, ethnic origin, marital status, geographical location, or any other group identity.
However, the
Sindh Population Policy, 2016
narrows the scope of access to FP services to married young people:
The Population Welfare Department will provide information, education and counseling on population issues and make available services for birth spacing to young married couples to minimize high risk fertility behaviours.
The latter policy references sociocultural beliefs surrounding young people
s reproductive health behaviors as justification for the focus on married youth. As such, the Population Policy overlooks the FP needs of unmarried youth, creating a barrier to access to services. Further, the Manual of Standards contradicts its own language on marital status cited above by stating:
Adolescents who are married need access to safe and effective contraception.
Because Sindh
s policy language favors married couples
access to family planning but does not restrict unmarried youth from accessing services, Sindh is placed in the yellow category for this indicator.
The
Manual of National Standards for Family Planning, 2009
and the
Manual of Standards for Family Planning Services, Sindh: Revised, 2017
discuss the special contraceptive and counseling needs of adolescents, ultimately encouraging providers to offer a full range of methods to youth:
Adolescents who are married need access to safe and effective contraception.
Many adolescents use no contraception or use a method irregularly, so they
are at high risk of unwanted pregnancy, unsafe abortion, and STIs [sexually transmitted infections]. In general,
adolescents are eligible to use any method of contraception. Services should
avoid unnecessary procedures that might discourage or frighten teenagers, such
as requiring a pelvic examination when they request contraceptives.
These policies align with the World Health Organization
s medical eligibility criteria and classify all short- and long-acting reversible methods as
use method in any circumstance
or
generally use method
for post-menarche women under age 18 and nulliparous women. Sindh is placed in the green category for this indicator.
Although the availability of emergency contraception (EC) is not factored into the categorization of this indicator, it is worth noting that the
Manual of National Standards
includes women of reproductive age in the eligibility requirement for EC and acknowledge youth vulnerability to sexual assault, which warrants the provision of this method:
While all women in situations of conflict are vulnerable to sexual assault, young female adolescents may be the group most in need of EC services. Adolescent refugees are often targeted for sexual exploitation and rape, yet there are relatively few programmes that address the specific reproductive health needs of young people, and even fewer that provide EC.
The
National Vision for Coordinated Priority Actions to Address Challenges of Reproductive, Maternal, Newborn, Child, Adolescent Health and Nutrition, 2016-2025
acknowledges the role that the national government can play in overseeing integration of reproductive health and family planning across sectors. The National Vision includes sexuality education for adolescents as one of the measures the Ministry of Health can support:
Focus on sexual & reproductive health education among adolescents, both boys and girls in school and out of school, is an important step that needs to be taken in a culturally sensitive manner.
However, the
Sindh Population Policy, 2016
limits the provision of sexuality education to married couples, using sociocultural beliefs as a justification. Under the
Focusing on Youth and Adolescents
section, the Population Policy emphasizes marriage as a precursor to parenthood, suggesting an abstinence-only educational approach:
Similar move would be initiated to support education of adolescents as their reproductive health issues are significant in urban and rural areas. However, this will be approached within the acceptable socio-cultural framework of the province and in conductive settings. As such, the Policy endorses that adolescents and youth may be equipped with knowledge about healthy and happy marital life leading to responsible parenthood.
Additional activities support educating older youth regarding life skills. Sindh addresses FP education for youth at the university level under Activity 5.4.1 of the
Costed Implementation Plan on Family Planning for Sindh, 2015
:
Consultations held with Department of Education, Health Education Commission, professional colleges to include life skills into the curriculum
Although the Costed Implementation Plan recognizes the provision of sexuality education, the scope is limited to college-age students. However, the
Sindh Reproductive Healthcare Rights Act, 2019
has provisions on reproductive health education in the curriculum at secondary and higher secondary school levels.
The
Sindh Youth Policy, 2018
indicates support for youth access to RH information. It incorporates short-term and mid-term strategies for education and communication activities at the school level and long-term strategies, including a
Youth Helpline
for counseling adolescents on SRH. The Youth Policy also affirms that the youth would be entitled to gender responsive and age-appropriate life skills-based education, both in school and out of school. However, further details of how the strategies would be implemented are not provided.
While some policies support youth access to information, other policies limit comprehensive sexuality education to married couples and focus on an abstinence-only educational approach, limiting the ability of youth to make positive sexual and reproductive health decisions. Sindh is placed in the red category for this indicator.
The provision of contraception to youth is highlighted as a special area of focus in the
Sindh Health Sector Strategy, 2012-2020
:
Strategy 3.4: Re-defining links with DoPW (Department of Population Welfare) with shift of contraceptive services through district and urban PHC [primary health care] systems and aimed at birth spacing in younger couples
The strategy includes an activity to integrate FP service provision with maternal care, which states that contraceptives should be provided at no cost to younger couples:
Integrating contraception provision: Provision of free contraceptives and training by DOPW to all DOH [Department of Health] facilities for birth spacing. Integration of services with pregnancy care to reach out to couples and supported by community-based BCC [behavior change communication].
The
Manual of Standards for Family Planning Services, Sindh: Revised, 2017
defines YF services and provides a checklist for facility observation that includes whether services are free or affordable to young people and whether several provisions to ensure privacy and confidentiality are in place.
The
Costed Implementation Plan on Family Planning for Sindh, 2015
identifies youth as a vulnerable segment of the population and acknowledges that strategies to reach this group include comprehensive and nonjudgmental contraceptive counseling and service provision. The Costed Implementation Plan includes activities to train health providers in YF service provision:
During the training of providers and community-based workers on FP, youth-friendly services and engagement will be added as a compulsory element of training (in-service and pre-service). Such an orientation of providers to the principles of youth-friendly services will allow existing facilities and community-based workers to incorporate ownership of providing services to meet the needs of young people.
The
Sindh Reproductive Healthcare Rights Act, 2019
includes language guaranteeing privacy during the provision of reproductive health services and ensuring the confidentiality of personal information:
(g) training of reproductive health care providers to be gender sensitive and to reflect user perspective to the right to privacy and confidentiality and also training in interpersonal and communication skills;
...
(k) provision of reproductive healthcare services to persons in privacy and ensuring personal information given thereof is kept confidential; .
Because these policies emphasize youth-friendly FP services and includes the three service-delivery elements
cost, privacy and confidentiality, and provider training
Sindh is placed in the green category for this indicator.
The
Costed Implementation Plan on Family Planning for Sindh, 2015
highlights reaching youth as a key concern and priority area. As a part of the discussion on reaching youth, the plan recognizes the importance of engaging the community to support youth access to FP:
Engagement with key gatekeepers and community leaders to foster an enabling environment for service uptake.
However, additional guidance on how this activity will be implemented, as well as discussion of approaches to address gender norms, are missing. While the
Sindh Youth Policy, 2018
includes a medium/ long-term strategy to sensitize youth groups regarding gender equality, it does not address gender norms specific to youth family planning.
Sindh is placed in the yellow category for this indicator.
The right of young people and adolescents to freely access family planning services without requiring consent from a parent or spouse is situated prominently in the
National Family Planning Guidelines and Standards, 2013
:
Decisions about contraceptive use should only be made by the individual client. No parental or spousal consent is needed for an individual to be given family planning information and services, regardless of age or marital status.
Given this clear declaration protecting youth autonomy in sexual and reproductive health decisionmaking, Tanzania is placed in the green category for this indicator.
The
National Standards for Adolescent Friendly Reproductive Health Services, 2004
affirm the rights of youth to access FP services and providers
obligation to adhere to youth rights:
All adolescents are informed of their rights on sexual and reproductive health information and services whereby these rights are observed by all service providers and significant others.
The
National Family Planning Guidelines and Standards, 2013
provide specific guidance to providers to deliver respectful, competent, and non-judgmental services to youth:
Standard 5.4: Service providers in all delivery points have the required knowledge, skills, and positive attitudes to effectively provide sexual and reproductive health services to young people in a friendly manner.
The service providers exhibits the following characteristics:
- Has technical competence in adolescent-specific areas.
- Respects young people.
- Keeps privacy and confidentiality.
- Allows adequate time for client/provider interaction.
- Is non-judgmental and considerate.
- Observes adolescent reproductive health rights.
The
National Adolescent Health and Development Strategy, 2018-2022
highlights provider bias and attitude as key barriers to youth access to family planning (FP) services, defining adolescent-friendly services as those that include:
Providers who are non-judgmental and considerate, easy to relate to and trustworthy [;] provide information and support to enable each adolescent to make the right free choices for his or her unique needs.
Taken together, these statements supporting youth access to sexual and reproductive health services free from provider judgment or bias indicate a supportive and favorable policy environment. Therefore, Tanzania is placed in the green category for this indicator.
The
National Standards for Adolescent Friendly Reproductive Health Services, 2004
makes a clear age-based statement protecting the rights of youth to access FP services:
All adolescents are informed of their rights on sexual and reproductive health information and services whereby these rights are observed by all service providers and significant others.
The
National Family Planning Guidelines and Standards, 2013
also directly mention the right of youth to receive FP services:
Like persons of other age groups, young people have the rights to decide if and when they want to have children, be informed and obtain information about family planning services, and access a full range of contraceptive methods.
Tanzania is placed in the green category for this indicator because its policies explicitly acknowledge young people
s right to FP services.
Standard 5.3 of the
National Family Planning Guidelines and Standards, 2013
recognizes the right of all young people to receive FP services, regardless of marital status:
Young people are able to obtain family planning services without any restrictions, regardless of their marital status.
With a clear recognition of married and unmarried youth
s right to FP services, Tanzania is placed in the green category for this indicator.
The
National Family Planning Guidelines and Standards, 2013
affirm the right of young people to access a full range of FP methods and direct providers to offer FP services in accordance with the World Health Organization
s medical eligibility criteria:
Contraceptives should be provided to clients in accordance with nationally approved method-specific guidelines, as defined by the World Health Organization (WHO) Medical Eligibility Criteria (MEC).
In addition to stating the right for youth to access family planning services, the
Guidelines and Standards
further acknowledges that youth have the right to access a full range of methods and references the
National Family Planning Procedure Manual, n.d.,
which details the WHO
s medical eligibility criteria allowing young people to access long-acting reversible contraceptives. Tanzania is therefore placed in the green category for this indicator.
Although the availability of emergency contraception is not factored into the categorization of this indicator, note that emergency contraception is included in the package of contraceptive offerings listed in the Procedure Manual.
The Ministry of Education and Culture in Tanzania has taken a broad stance on the form of sexuality education to offer to youth. The Ministry developed the
Guidelines for Implementing HIV/AIDS/STDs and Life Skills Education in Schools and Teachers
Colleges, Version 2, 2002
as a response to increased HIV transmission among youth. As a result, the directives focus primarily on the prevention of HIV and sexually transmitted infections. Comprehensive sexuality education (CSE), specifically, is not referenced and accordingly not defined.
The Guidelines describe the national approach to sexual education as:
The content of HIV/AIDS/STIs control education shall aim at developing and promoting knowledge, skills positive and responsible attitudes such as assertiveness, effective communication, negotiation, informed decision making and provide motivational support as a means to responsible sexual behaviour.
These guidelines were developed in 2002, prior to the publication of international guidance on CSE. This framing is not comprehensive and limits the provision of information on sexuality, safe sexual behaviors, sexual and reproductive health (SRH) care, and gender.
To promote a holistic approach to life skills education, including self-awareness, relationship skills, cognitive skills, and SRH education, Tanzania developed the
National Life Skills Education Framework, 2010.
The Framework notes that despite concerns from stakeholders who contributed to the content, health-based life skills would be covered in biology and governance entrepreneurship courses, and that life-skills education will be
de-linked from an exclusive emphasis on SRH and HIV/AIDS.
The education would have a
strong gender orientation
and will ensure that
students get a sufficient
dose
of SRH/HIV education [but] they will also be taught to apply life skills to other areas in sufficient depth to have an impact.
Additional policies implicitly acknowledge the limitations of the current policy environment for CSE. The
National Adolescent Health and Development Strategy, 2018-2022
recommends:
Promote a comprehensive curriculum which makes sexual and reproductive health, nutrition, life skills and empowerment compulsory topics to be included in secondary school and non-formal education packages.
The
National Family Planning Costed Implementation Plan 2019-2023
supports the adoption of policies that improve youth access to contraceptive information and services and integrates a CSE program into the national curriculum.
One of the Costed Implementation Plan's strategic outcomes is to adopt and implement policies that improve access to high-quality FP information for in-school youth:
OUTCOME 2: Adopt and implement policies that improve equitable and affordable access to high-quality FP services and information
Stakeholders identified two opportunities to reach in-school youth: 1) reviewing and rolling out an evidence-based national comprehensive sexual education curriculum to ensure that the content on contraception is strong and evidence-based and 2) revising the National School Health Programme guidelines and strategy to include FP information.
Output EE 4: Policies supporting young people
s access to contraceptive information and services adopted and implemented.
Activity 1: Include strong, evidence-based FP content into Comprehensive Sexuality Education (CSE), currently integrated in national school-based curricula for primary and secondary schools.
The Costed Implementation Plan
s strategic outcome to increase total demand for contraception also acknowledges the need to tailor communication materials and channels to reach target audiences, namely youth, with FP information. The Costed Implementation Plan aims for these messages to focus on providing accurate and relevant information about FP methods, promoting the availability of FP services and the importance of healthy timing and spacing of births, and ensuring that audiences are aware of their rights related to FP services.
While the Costed Implementation Plan activity includes sub-activities detailing the necessary steps for the adoption of a new CSE curriculum, including stakeholder workshops and costing for drafting, revision, and dissemination of the policy, it does not include guidelines that are fully aligned with the United Nations Population Fund
s (UNFPA
s) essential components. To improve upon existing guidelines, the Ministry of Education and Culture should consider including the nine essential components for CSE in any future curricula revisions. Tanzania is placed in the yellow category for this indicator.
The
National Road Map Strategic Plan to Improve Reproductive, Maternal, Newborn, Child, and Adolescent Health in Tanzania, 2016-2020 (One Plan II)
prioritizes adolescent and youth-friendly (YF) family planning services, setting a target to increase the proportion of adolescent and YF health services from 30%to 80%by 2020. The
National Family Planning Costed Implementation Plan, 2019-2013
includes provider training and ensures confidentiality and privacy within its activities to improve availability and access to quality YF services:
OUTPUT SD4: Number of facilities offering quality youth-friendly services according
to established national youth-friendly service standards increased
Reflecting strategic priority 4, activities in this output focus on improving services for young
people at both the facility and community levels. First, an assessment will be conducted with youth of different profiles (e.g., different age groups, married versus unmarried, in- versus out-of-school) to collect information regarding barriers they face in accessing contraceptive services. Findings will be shared with CHMTs [Council Health Management Teams] and facility managers as part of advocacy to prioritise funding for structural changes, including infrastructure improvements to ensure privacy and confidentiality, changes in hours of service, and signage to publicise facilities that have undertaken efforts to become adolescent-friendly. Facilities will be identified for improvement and for training needs via routine supervision. In collaboration with the Adolescent and Reproductive Health Unit, at least one trainer per region will be trained in YFCS [youth-friendly contraceptive services]. At least two providers per facility across the country will be trained to offer contraceptive services to youth without bias or barriers; these trainings will also include private facilities or pharmacies and ADDOs [accredited drug dispensing outlets] that youth are likely to frequent. In addition, operators of the youth-focused toll-free help line will also be trained in YFCS. In addition to showing visible signs that identify them as meeting requirements for YFCS, facilities will be included in a YFCS directory that can be disseminated through FP stakeholder meetings, trainings, and zonal meetings and through the toll-free help line. Efforts will also be made to reach young people with services outside of facilities, including outreach from facilities to places where youth gather frequently (e.g., youth clubs, youth corners). The quality of YFCS offered by both facility- and community-based providers will be assessed during routine supportive supervision visits conducted under Output SD1.
The Tanzania
National Family Planning Guidelines and Standards, 2013
recognize the unique FP needs of young people as a group deserving special consideration:
All family planning service-delivery points
whether in a facility, community, or outreach setting
should incorporate youth-friendly services, as further described in Section II: Standards. Services are youth-friendly if they have policies and attributes that attract youth to the services, provide a comfortable and appropriate setting for serving youth, meet the needs of young people, and are able to retain their young clients for follow-up and repeat visits.
This document further details specific directives for the provision of YF services (Standard 5.1.-5.6.), provider training, and free contraceptives for all FP clients in the public sector.
Together, these policies address each of the three service-delivery core elements that improve adolescent and youth uptake of contraception. Therefore, Tanzania is considered to have a supportive and favorable policy environment surrounding service provision and is placed in the green category for this indicator.
The
National Family Planning Costed Implementation Plan, 2019-2023
outlines activities to lead to positive shifts in social norms and attitudes, with the goal of fostering healthier behavior and beliefs around contraception:
Given that the FP Goals Model identified improving social norms related to FP as a major contributor to future mCPR [modern contraceptive prevalence rate] growth, specific attention will be paid to identifying and subsequently addressing and shifting social norms. The foundation activity will be an assessment to identify social norms that currently impede FP use in the priority 18 regions, the findings of which will inform subsequent activities in this and other outputs.
Developed messages will be tailored to address specific norms relevant for the specific regions and groups, including messages targeted to health care providers to normalise FP services for all age groups. The messages and tools will be integrated into community-sensitisation activities run by CHWs [community health workers] and shared with local FP champions. CHWs who underwent the government
s one-year training for CHWs, and who will be identified through mapping conducted under the service delivery thematic area, will receive refresher training and support to conduct community-mobilisation activities using updated content to change social norms and attitudes (i.e., module 1 of the FP refresher training curriculum). A message development guide and tailored messages will be part of the service delivery supervision conducted monthly by nearby health facilities. Also, in collaboration with a media consultant, messages that address social norms will be developed for local radio, while messages that address
shared
norms (across regions) will also be aired through national radio.
While not specific to contraceptive services, the
National Adolescent Health and Development Strategy, 2018-2022
emphasizes community engagement and efforts to overcome gender norms:
Misinformation among gatekeepers is a potential drawback to adolescents
access to health services as parents, guardians and local leaders are critical information channels for adolescents
By empowering families and the community in general, demand for adolescent friendly health services can be significantly improved.
Among its top priorities and recommendations, the Strategy aims to:
Create strong linkages with community groups, community-based organizations [CBOs] and faith-based organizations [FBOs] to promote positive socio-cultural norms.
The Strategy also notes gender norms
impact on adolescent health:
Gender norms have an influence on the health of adolescents, which manifests through discrimination of both male and female adolescents, leading to marginalization
Contradictory gender norms from family and society can shape sexual expectations with implications on engagement in unsafe sexual behaviors.
Gender norms are briefly referenced within the Strategy
s strategic recommendations, which include a call to raise the minimum age at marriage to 18:
CBOs and FBOs should also address gender norms, roles and relationships that may be harmful
Cash transfer interventions can particularly help adolescent girls take fewer risks in their sexual relationships.
The
National Road Map Strategic Plan to Accelerate Reduction of Maternal, Newborn, and Child Deaths in Tanzania, 2016-2020 (One Plan II)
includes several activities to use community support for adolescent and youth sexual and reproductive health, including:
Activity 5.5: Support utilization of existing community structures (religious leaders, parents, community and government leaders) to reach young people with age-appropriate sexual and reproductive health information and link them to services.
Tanzania is placed in the green category for this indicator since its strategies not only acknowledge the importance of engaging the community in the provision of FP services to youth, but also identify interventions to build community support for youth-friendly FP services and address gender norms.
Togo
s policy environment does not explicitly prohibit parental or spousal consent. Togo is placed in the gray category for this indicator.
The
Protocoles de sant
de la reproduction ; sant
de la m
re, sant
de l
enfant, sant
des jeunes et adolescents(es), sant
des hommes
; tome I ; 2
dition, 2009
make clear that providers should be nonjudgmental of youth:
1.2- Ce qu
il ne faut pas faire
- S
imposer d
embl
e lorsqu
on engage une discussion avec les jeunes.
- Ridiculiser les jeunes.
- Juger les jeunes.
-
tre n
gatif ou pessimiste lorsqu
on travaille avec les jeunes.
- Sous-estimer la capacit
des jeunes.
Comment les adolescents et jeunes aimeraient
tre trait
s?
- Les acceptez tels qu
ils sont, ne pas leur faire de la morale et ne pas les d
moraliser
- ...Ne pas les juger.
The
Loi n
2007-005 sur la sant
de la reproduction, 2007
guarantees the right of reproductive health to adolescents without discrimination. Similarly, the
Politique et normes en sant
de la reproduction, planification familiale et infections sexuellement transmissibles de Togo, 2009
state that providers should withhold judgment when counseling clients on FP methods:
2- LES CLEFS D
UN BON COUNSELING
CHAPITRE 2 : LE COUNSELING EN PF
- Montrer du respect et de l
amabilit
envers le (la) client(e) par son approche sans jugement,
- Ecouter activement les pr
occupations du (de la) client(e),
- Pr
senter l
information sans partie pris dans le respect du sentiment du (de la) client,
CHAPITRE 2 : LE COUNSELING EN PF
.
3.4- Choix/ D
cision
- Aider le (la) client(e)
choisir la m
thode qui lui convient,
- Rester neutre,
- Discuter des crit
res d
ligibilit
du (de la) client(e),
- S
assurer que le (la) client(e) est bien inform
(e),
Because Togo
s policies explicitly state that providers must avoid judgment of youth when providing FP, Togo is placed in the green category for this indicator.
The
Loi n
2007-005 sur la sant
de la reproduction, 2007
states that reproductive health services should be available to all individuals regardless of age or marital status and further guarantees adolescents
right to reproductive health without discrimination:
Art. 7 - En mati
re de sant
de la reproduction, tous les individus sont
gaux en droit et en dignit
sans discrimination aucune fond
e sur l'
ge, le sexe, le revenu, la religion, l'ethnie, la race, la situation matrimoniale ou sur toute autre situation touchant
l'
tat de la personne.
Art. 9 - Le droit
la sant
de la reproduction est reconnu, sans discrimination aucune,
tout individu, personne du troisi
ge, adulte, jeune, adolescent et enfant.
Similarly, the
Politique et normes en sant
de la reproduction, planification familiale et infections sexuellement transmissibles de Togo, 2009
state that youth-friendly services are based on the principle that adolescents have the right to health services regardless of age:
Le respect des droits humains et en particulier le droit des adolescents/jeunes
s aux services de sant
de qualit
sans discrimination aucune li
leur
ge, leur sexe, leur religion ou condition sociale
Togo is placed in the green category for this indicator.
The
Loi n
2007-005 sur la sant
de la reproduction, 2007
guarantees the right to reproductive health services
including FP
regardless of age or marital status and further guarantees the right to reproductive health to adolescents without discrimination:
Art. 7 - En mati
re de sant
de la reproduction, tous les individus sont
gaux en droit et en dignit
sans discrimination aucune fond
e sur l'
ge, le sexe, le revenu, la religion, l'ethnie, la race, la situation matrimoniale ou sur toute autre situation touchant
l'
tat de la personne.
Art. 9 - Le droit
la sant
de la reproduction est reconnu, sans discrimination aucune,
tout individu, personne du troisi
ge, adulte, jeune, adolescent et enfant.
The
Programme national de lutte contre les grossesses et mariages chez les adolescents en milieux scolaire et extrascolaire au Togo, 2015-2019
includes a focus on access to improving sexual and reproductive health services and targets both married and unmarried youth:
Axe strat
gique 3 : Acc
information et aux services de sant
sexuelle et de la reproduction adapt
s aux adolescents
R
sultat d
effet 3.1
Un plus grand nombre d
adolescentes utilisent de services contraceptifs.
- % d
adolescentes (15
19 ans) mari
es utilisant une m
thode moderne de contraception
- % d
adolescentes (15
19 ans) non-mari
es utilisant une m
thode moderne de contraception
Togo is placed in the green category for this indicator because its policy environment protects youth access to family planning regardless of marital status.
The
Standards de services de sant
adapt
s aux adolescents et jeunes de Togo, 2009
describe the package of minimum services for adolescents at each level of the health system, which includes all methods of contraception, including long-acting reversible contraceptives (LARCs). The
Protocoles de sant
de la reproduction du Togo ; composantes communes, composantes d
appui
; tome II ; 2
me edition, 2009
include a full range of contraceptive options for youth in FP services and acknowledge the importance of providing contraception to sexually active youth. However, the policy states that abstinence should be strongly recommended to adolescents. It includes restrictions for recommending intrauterine devices (IUDs) to adolescents based on parity, frequency of sexual activity, and number of partners:
Appliquer la conduite
tenir :
convient
ou ne convient pas
en tenant compte des caract
ristiques de l
adolescent et de son choix
| Caract
ristiques |
M
thode de choix |
M
thode
non appropri
e |
| Nulligeste |
Pilules combin
es |
DIU |
| Partenaires multiples |
Pr
servatifs |
DIU |
| Inconscience |
DIU |
Pilule |
| Cycles irr
guliers |
Pilule combine |
PSP
injectable |
| Rapports sexuels occasionnels espac
s ou irr
guliers |
Pr
servatifs Spermicides |
DIU |
...
7- PROGRAMMER LES VISITES SELON LA METHODE CHOISIE
N.B. Une sexualit
coce augmente le risque de cancer du col. L
abstinence devrait
tre fortement recommand
e chez un adolescent
The
Plan d
action national budg
de planification familiale du Togo, 2017-2022
includes as one of its main objectives offering a varied and complete range of contraceptive methods, with a focus on youth:
Objectif 2 : Garantir l
offre et l
des services de PF de qualit
en renfor
ant la capacit
des prestataires publics, priv
s et communautaires et en ciblant les jeunes dans les zones rurales et les zones enclav
es par le biais de l
largissement de la gamme des m
thodes, y compris la mise
chelle des MLDA [m
thode
longue dur
action], la PFPP [planification familiale post-partum] et l
lioration des services destin
s aux jeunes.
While some Togolese policies support youth access to a full range of methods, the existence of the
Protocoles de sant
de la reproduction: tome II, 2009
restricting the provision of LARCs to youth places Togo in the red category. Future protocols for provider provision of LARCs for adolescents should be updated based on the most recent World Health Organization medical eligibility criteria for contraceptive use.
Although the availability of emergency contraception is not factored into the categorization of this indicator, note that the
Protocoles de sant
include emergency contraception in the general list of contraceptive methods, but not in the adolescent-specific section on sexual and reproductive health. Thus, it is not clear whether the policy intends for emergency contraception to be accessible to youth.
The
Loi n
2007-017 portant code de l'enfant, 2007
guarantees every child the right to information on reproductive health:
- Le droit de tout enfant d'avoir des informations sur la sant
de la reproduction.
The
Loi n
2007-005 sur la sant
de la reproduction, 2007
states that everyone has the right to information and education on sexual and reproductive health:
Art. 13 - Tout individu a droit
l'information,
l'
ducation utile
sa sant
sexuelle et reproductive et aux moyens n
cessaires lui permettant d'
valuer les avantages et les risques pour un choix judicieux.
The
Plan national de d
veloppement sanitaire, 2017-2022
lists comprehensive sexuality education (CSE) and information, advice, and services for sexual and reproductive health, including commodities, as priority interventions for adolescent health and development.
Orientation strat
gique : Promotion de la sant
et le d
veloppement de l
adolescent
Renforcement du cadre de concertation intersectoriel en mati
re de promotion de la sant
des adolescents ;
-
ducation sexuelle compl
te ;
- Informations, conseil et services pour une sant
sexuelle et g
sique compl
te, contraception incluse ;
The
Plan d
action budg
de la planification familiale au Togo, 2017-2022
includes activities to reach youth in formal and informal settings, which is one of the essential components of CSE:
CD2-A4. Harmonisation des curricula d
enseignement sur l
ducation sexuelle compl
te dans les syst
mes
ducatifs (formel et informel)
Actualiser les connaissances sur la SRAJ [sant
reproductive des adolescents et des jeunes dans les
coles gr
ce aux nouveaux modules d
ducation sexuelle compl
te dans les curricula de formation. Des enseignants exp
riment
s seront form
s pour
tre des formateurs. Ils animeront ensuite des sessions de formation des formateurs chaque ann
e. Ces derniers assureront l
ducation sexuelle compl
te des adolescents et jeunes.
Similarly, the
Programme national de lutte contre les grossesses et mariages chez les adolescents en milieux scolaire et extrascolaire au Togo, 2015-2019
includes specific activities for introducing CSE to youth, particularly girls, in and out of school:
Axe strat
gique 2 : Acc
s et maintien des adolescentes dans le syst
ducatif et acc
ducation sexuelle compl
te
Il vise
galement l
ducation sexuelle compl
te (ESC) pour toutes les adolescentes en milieux scolaire et extrascolaire. L
ESC est reconnue globalement comme une strat
gie efficace pour pr
venir les grossesses pr
coces et renforcer l
autonomisation des adolescentes.
R
sultats d
effet 2.2 : La qualit
et la couverture de l
ducation sexuelle compl
te sont renforc
es dans les
tablissements scolaires, dans les centres de formations professionnelles et pour les portefaix, les domestiques et les serveuses dans les bars
As part of its gender approach, the
Politique et normes en sant
de la reproduction, planification familiale et infections sexuellement transmissibles de Togo, 2009
includes a plan to incorporate gender into population education for youth, another of the essential components of CSE:
En mati
re d'
ducation des enfants, des adolescents et des jeunes, il s'agira d'introduire des modules d'approche genre dans l'EPD [
ducation en mati
re d'environnement et de population pour un d
veloppement humain durable] / SR [sant
de reproduction]..
The "Plan d
action pour le repositionnement de la planification familiale au Togo, 2013-2017" includes strategies for improving communication on family planning services to adolescents and young people. While strategies include using new technologies such asradio and television broadcasts to target adolescents and young people in school and out of school, the
Plan d
action
does not clarify whether the communication will include essential components of CSE.
Togo
s policy environment is supportive of CSE but does not reference all nine of the United Nations Population Fund
s (UNFPA
s) essential components of CSE. Togo is placed in the yellow category for this indicator.
The
Plan d
action pour le repositionnement de la planification familiale au Togo, 2013 -2017
includes a strategy to improve the supply of FP services for adolescents and young people in and out of school through capacity building of providers.
Strat
gie O6 : Am
lioration de l
offre des services de PF [planification familiale] offerts en direction des adolescents et jeunes
Mieux int
grer les sp
cificit
s des adolescents et des jeunes
travers des interventions mieux adapt
leurs besoins en mati
re de SSR [sant
sexuelle et de reproduction] /PF, qu
il s
agisse des jeunes scolaris
s ou des jeunes non scolaris
s. Ceci n
cessite le renforcement de la capacit
des prestataires et la mise en place d
une ligne verte accessible aux adolescents et aux jeunes.
Activit
O6.1 : Renforcement des capacit
s des prestataires de 25% des FS [formations sanitaires] pour offrir les services de PF adapt
s aux adolescents et aux jeunes.
Renforcer les capacit
s des prestataires de 25% des FS (168 FS sur 674 FS offrant d
la PF) pour offrir les services de PF adapt
s aux adolescents et aux jeunes de 34 FS (
raison de 2 personnes
former par FS) par ann
e de 2013
2017.
- Recensement des FS appropri
es pour la prise en charge des adolescents et jeunes
- Adaptation des manuels de formation en prise en charge des jeunes et adolescents dans les FS
- Organisation de 3 sessions de formation de 2 personnes par FS pendant 5 jours en prise en charge des jeunes chaque ann
e de 2013
2017
- Suivi des activit
s de formation
The
Protocoles de sant
de la reproduction ; sant
de la m
re, sant
de l
enfant, sant
des jeunes et adolescents(es), sant
des hommes
; tome I ; 2
me edition, 2009
describe the necessary characteristics of provider interactions with adolescents, such as respecting their moral principles, establishing a climate of trust, and ensuring confidentiality:
Ils ont besoin d
attention et de compr
hension, d
la n
cessit
de d
velopper une approche amicale avec eux dans le but d
tablir un climat de confiance, de dialogue confidentiel et de respect de leurs principes moraux et de cr
er un service adapt
leur prise en charge.
The
Plan d
action national budg
de la planification familiale du Togo, 2017-2022
includes plans to train providers in youth-friendly FP service provision and specifically targets removing the obstacle of negative provider attitudes:
OA1-A12. Mise en place des services de SR [sant
de la reproduction /PF adapt
s aux jeunes et les adolescents, ind
pendamment de leur statut et lieu de r
sidence
Sur la base du diagnostic de la PF au niveau des jeunes, il s
agit de mieux int
grer les sp
cificit
s des adolescents (es) et jeunes
travers des interventions mieux adapt
leurs besoins en mati
re de contraception, qu
il s
agisse des jeunes scolaris
s ou non scolaris
s, du milieu rural ou urbain. Ceci n
cessite le renforcement de la capacit
des prestataires, le renforcement des lignes vertes int
grant le volet PF et accessibles aux adolescents (es) et jeunes ainsi que la promotion d
activit
s int
es de PF, de lutte contre le VIH et le sida voire de prise en charge des des IST [infections sexuellement transmissibles] chez les jeunes...
OA2-A5. Renforcement des capacit
s des prestataires des FS en offre de services conviviaux et adapt
s de SRAJ [sant
reproductive des adolescents et des jeunes] y compris la contraception
Renforcer les capacit
s des prestataires de 10% des FS publiques (soit 77 FS sur 768 FS offrant la PF) par an dans le domaine de l
offre des services de PF adapt
s aux adolescents et jeunes. Ceci permettra de lever l
obstacle li
attitude inappropri
e des prestataires face aux adolescents et jeunes qui se pr
sentent dans les centres de sant
pour adopter les m
thodes de PF. Elle sera r
alis
travers la formation, l
nagement des structures de soins, la supervision et le suivi des prestations.
The
Plan d
action
aims to offer free FP services during national family planning weeks and youth days at health facilities. The
Standards de services de sant
adapt
s aux adolescents et jeunes de Togo, 2009
aim to improve the financial accessibility of youth-friendly services, and the
Programme national de lutte contre les grossesses et mariages chez les adolescents en milieux scolaire et extrascolaire au Togo, 2015-2019
includes an activity to pilot a contraceptive subsidy program for adolescents. The most recent
Plan national de d
veloppement sanitaire, 2017-2022
includes the development of FP services specific to young people and adolescents as a priority intervention.
Togo is placed in the green category for this indicator because all three youth-friendly service-delivery elements are addressed.
One of the five standards in
Standards de services de sant
adapt
s aux adolescents et jeunes de Togo, 2009
seeks community support for health services adapted to youth:
Standard 4 : Les membres de la communaut
et les associations communautaires y compris les adolescents et les jeunes sont organis
s en vue de faciliter l
utilisation des services de sant
par les adolescents et les jeunes
The
Programme national de lutte contre les grossesses et mariages chez les adolescents en milieux scolaire et extrascolaire au Togo, 2015-2019
, which explicitly aims to extend youth access to contraception, includes activities for building community support for preventing adolescent pregnancies. These activities include engaging community leaders and community-based organizations:
R
sultat d
effet 4.2 : Les parents, les communaut
s et les leaders traditionnels et religieux s
engagent dans la lutte contre les grossesses et mariages des adolescentes
R
sultats d
effet 4.3 : Les OSC [Organisations de la Soci
Civile]/OBC [Organisations de Base Communautaire] sont plus aptes
intervenir efficacement dans la pr
vention et la prise en charge des grossesses et mariages chez les adolescentes
The
Politique nationale pour l'equit
et l'
galit
de genre du Togo, 2011
plans to raise awareness of gender issues among health stakeholders and to integrate a gender approach into sexual and reproductive health services for men, women, and adolescents:
Objectif 3.2. Assurer la prise en compte des besoins diff
renci
s en sant
de la reproduction des femmes, des adolescent(e)s et des hommes
- Int
gration effective de l
approche genre dans la conception la planification, la budg
tisation des interventions en sant
et SR [sant
de la reproduction]
- Mener des activit
s de sensibilisation et de plaidoyer des acteurs du secteur sant
sur les questions de genre et leurs manifestations sur la sant
et la SR des femmes et des hommes et des adolescent(e)s
Togo is placed in the green category for this indicator because its policies include a detailed strategy for building an enabling social environment.
Uganda
s policy environment supports youth access to FP services without authorization by a third party. The
National Policy Guidelines and Service Standards for Sexual and Reproductive Health and Rights, 2006
explicitly affirm the right of all people, including youth, to access FP services without parental or spousal consent:
No verbal or written consent is required from parent, guardian or spouse before a client can be given family planning service except in cases of incapacitation (intellectual disability). Clients should give written consent to long-term and permanent family planning methods.
Uganda is placed in the green category for this indicator.
The
Uganda Clinical Guidelines 2016: National Guidelines for Management of Common Conditions
instructs providers to counsel clients to make voluntary, informed FP choices. Providers are directed to explain each method using the medical eligibility criteria:
Help client choose appropriate method using family planning medical eligibility criteria wheel
The medical eligibility criteria for contraception in Uganda specify that youth are eligible for short-term methods and long-acting reversible contraceptives. This provides a promising policy environment for provider authorization of youth FP services, but it would be strengthened with explicit guidance to providers to withhold personal judgment when offering these services. Uganda is placed in the yellow category for this indicator.
The
National Policy Guidelines and Service Standards for Sexual and Reproductive Health and Rights, 2006
explicitly mention the right of all Ugandans, regardless of age, to access family planning services:
Every individual who is sexually active can receive family planning and contraceptive services irrespective of age or mental status.
The acknowledgement of individuals
right to receive sexual and reproductive health services, regardless of age, signals a strong policy environment and warrants categorization the green category for this indicator.
The
National Policy Guidelines and Service Standards for Sexual and Reproductive Health and Rights, 2006
explicitly mention the right of all Ugandans to access FP services:
Every individual who is sexually active can receive family planning and contraceptive services irrespective of age or mental status.
While inclusive of all people, the policy does not explicitly recognize marital status as a criterion for provision or refusal of FP services. Providers and clients may differentially interpret this statement, potentially creating a barrier for youth desiring access to contraception. To strengthen the eligibility criteria, the guidelines eligibility statement should specifically recognize segmented parts of the population, such as married and unmarried youth. Because no policy exists addressing marital status in access to FP services, Uganda is placed in the gray category for this indicator.
The
National Policy Guidelines and Service Standards for Sexual and Reproductive Health and Rights, 2006
state that all sexually active Ugandans are eligible for family planning services:
All sexually active males and females in need of contraception are eligible for family planning services provided that:
They have been educated and counseled on all available family-planning methods and choices;
Attention has been paid to their current medical, obstetric contra-indications and personal preferences.
The eligibility criteria state that women of reproductive age, including adolescents, and nulliparous women can generally use each short-term (contraceptive pill and injectable) and long-acting reversible (intrauterine device and implant) methods. The same medical eligibility criteria are reinforced in the
Uganda Clinical Guidelines 2016: National Guidelines for Management of Common Conditions.
Uganda is placed in the green category for this indicator.
Although the availability of emergency contraception is not factored into the categorization of this indicator, note that the latter document includes adolescents in the eligibility for emergency contraception:
Emergency contraception indications: All women and adolescents at risk of becoming pregnant after unprotected sex.
The
National Sexuality Education Framework, 2018
aims to streamline the delivery of sexuality instruction in formal education settings by providing young people with
age-appropriate values and skills-based information about their sexuality in accordance with Uganda
s national, religious, and cultural values.
The framework promotes sexual abstinence outside of marriage and restricts sexual and reproductive health (SRH) information to students, in part due to religious opposition. The document also avoids any discussion of contraceptive use or family planning methods as a way to prevent unwanted pregnancies.
Strategic Priority Policy Goals and Outcomes for NSEF [National Sexuality Education Framework]: 3) To promote health behaviors such as sexual abstinence and health-seeking behaviors.
Since the current framework does not include the exact messaging that will be provided in schools, an opportunity exists for the National Curriculum Development Center to elaborate on important SRH information as the associated curriculum, textbooks, and messages are developed. However, the exclusion of critical sexuality education material and promotion of abstinence-only practices in this Framework suggests that the current policy environment creates a barrier to youth accessing care.
The
National Child Policy, 2020,
which addresses the welfare of Ugandans under age 18, discusses the provision of comprehensive SRH education as a priority action under their adolescent-friendly health services strategy:
Strategy 5: Improve provision of and access to Adolescent-Friendly Health Services (AFHS)
c) Promote behaviour change among adolescents through comprehensive sexual and reproductive health education, and life skills education through school and community-based interventions.
The policy includes another strategy to
improve access to SRHR [sexual and reproductive health and rights] education, HIV prevention, care, and treatment services for children and adolescents
but fails to include any priority actions that provide further detail on the content of SRHR education and how it would be provided.
New policies and future curricula should continue to incorporate the nine United Nations Population Fund (UNFPA) essential components of comprehensive sexuality education and must address or replace the emphasis on abstinence currently found in the Framework. Thus, Uganda is placed in the red category for this indicator.
Youth-friendly FP service provision features prominently across Uganda
s policy documents. While none of the policies detail clear action steps aligned with all three service-delivery core elements of adolescent-friendly contraceptive services, each recognizes the need to tailor services to youth.
The
Health Sector Strategic Plan III, 2010/11-2014/15
specifically targets adolescents and youth in the sexual and reproductive health (SRH) services strategy. The strategy proposes the following activities to strengthen adolescent SRH services and the policy environment surrounding SRH:
Strengthen adolescent sexual and reproductive health services:
- Integrate and implement adolescent sexual and reproductive health in school health programmes; and
- Increase the number of facilities providing adolescent friendly sexual and reproductive health services.
- Strengthen the legal and policy environment to promote delivery of SRH services.
- Review SRH and related policies and address institutional barriers to quality SRH services.
- Review SRH policies, standards, guidelines and strategies as need arises.
The
Uganda Family Planning Costed Implementation Plan, 2015-2020
includes a FP service delivery activity targeting youth:
SD9. Youth-friendly services are provided in clinics. To increase the availability of youth-friendly services, youth-friendly corners will be established, and health workers will be trained on youth-friendly services. In addition, FP service delivery hours will be increased to include outside school hours to accommodate youth.
The
National Multi-Sectoral Coordination Framework for Adolescent Girls, 2018-2022
outlines key interventions to train service providers to offer adolescent-friendly information:
Build capacity of service providers (health workers, teachers, community development officers, welfare officers) and institutions to offer adolescent responsive services including providing age appropriate information to adolescents, parents, caregivers and communities on nutrition, immunization, personal hygiene, general health seeking behavior and relevant pathways for referral.
Both activities mention providing training to providers on YF services but do not reference training providers to withhold personal beliefs, bias, or judgment when offering contraception services to youth.
Altogether, the strategies generally address providing youth-friendly FP services to youth but do not sufficiently incorporate all three service-delivery elements of adolescent-friendly contraceptive services, placing Uganda in the yellow category for this indicator. To bolster the policy environment supporting youth-friendly FP service provision, future guidelines should consider including the remaining service-delivery elements of adolescent-friendly contraceptive provision.
The
Uganda Family Planning Costed Implementation Plan, 2015-2020
includes comprehensive actions to create demand for FP services among youth, including elements of building community support:
DC3. Young people, 10-24 years old, are knowledgeable about family planning and are empowered to use FP services: To increase the knowledge and empowerment of young people, peer educators will be engaged and supported; media (print and online) targeting youth will be disseminated; and
edutainment
community events will provide the opportunity for knowledge exchange amongst young people and empower adults to help youth avoid teenage pregnancy.
The Plan's proposed steps not only target youth in awareness and mass media campaigns, but also seek to engage gatekeepers in additional community engagement activities:
Empower parents, caregivers, and teachers to help their children to avoid teen pregnancy, including improving parent-child communication on sexual issues.
The
National Child Policy, 2020
includes increasing access to and improving provision of reproductive and maternal health care services as one of its strategic actions aimed at preventing child mortality and promoting children
s health; children are defined in this policy as those under age 18. Within this strategic action, the policy lays out multiple priority actions that link service delivery with activities that build support in communities and address gender norms but are not specific to family planning:
5.1.1 Strategies and priority actions
Strategy 1: Increase access to and improve provision of reproductive and maternal health care services
c) Promote sexual reproductive health among young people
h) Strengthen family and community based support for women seeking appropriate care before and during pregnancy, delivery, and postpartum period.
i) Promote male involvement in positive social norm change, maternal and child health service planning and delivery
j) Advance community mobilization efforts to build capacity of women, families, and communities to actively engage with each other and with health providers and managers to improve the quality of services, and to hold health systems accountable.
The inclusion of a detailed strategic initiative to build community support among youth and adults for youth FP services in the Costed Implementation Plan indicates a promising policy environment, placing Uganda in the yellow category for this indicator. Outlining additional activities to address gender norms specific to family planning in future policies would make youth access to and use of contraception more acceptable and appropriate within their communities.
The
Zambia Family Planning Guidelines and Protocols, 2006
list specific strategies for incorporating family planning into adolescent reproductive health issues. The strategies acknowledge that current legislation allows youth FP access without parental and spousal consent but encourages spousal and parental counseling:
Facilitate access, especially for young girls, to all types of services dealing with RH [reproductive health] concerns and specifically FP, without consent of spouses, parents/guardians or relatives as allowed by current legislation. Spousal/guardian counselling, however, is strongly recommended. Special concern has to be given to the counselling of adolescents under 16 years of age. When, after counselling, young adolescents are unwilling to involve their parents/guardians, special care should be taken to ensure that these adolescents under 16 have the mental maturity to understand what is involved in their decision along with its possible consequences.
Zambia is placed in the green category for this indicator as its policies support youth access to family planning services without consent from parents and spouses.
The
Zambia Family Planning Guidelines and Protocols, 2006
lay out service delivery requirements for quality of care in family planning and notes that providers must not interfere in method choice with their personal opinions or preconceived biases:
Choice of Methods
All women, men, and young people shall be provided with the FP methods they request, subject to them meeting the agreed eligibility criteria, without the interference of personal opinions or preconceived biases of the service providers.
The Guidelines and Protocols go on to detail principles of a client-provider relationship and although not specific to youth, note that providers should:
- Ensure that providers communicate with clients effectively and in culturally appropriate ways.
- Treat all clients with respect and dignity.
- Provide quality services in a way that does not infringe upon the client's rights.
- Personalize care so that it is responsive to the client's needs and is not influenced by personal biases.
- Assure privacy and confidentiality.
Zambia is placed in the green category for this indicator as its policies address provider authorization for FP services.
The age of consent for various sexual and reproductive health (SRH) services has been identified as an ongoing issue in Zambia, with policies and legal frameworks providing conflicting information.
The
Adolescent Health Strategy, 2017-2021
acknowledges this weakness in the policy environment and notes the unavailability of adolescent-responsive SRH health services in all health institutions, with access to existing services limited to ages 16 and above. The strategy identifies review and alteration of the age of consent
from the current 16 to lower
and sets aside funding for age-of-consent policy and guideline development:
Activity:
Policy and Guidelines development
Costing Estimates per activity (US$):
Review of policy and development of guidelines
Estimated Cumulative Calculation:
$20,000 for review and development and dissemination of policy guidelines on age of consent and access to SRH services
Total Expansion Districts & Health Center (H/C) or by Frequency:
$20,000 for review and revision of guidelines for care and support for adolescents to transition from pediatric to adult clinical care
Total over 5 years:
$40,000
Zambia
s policies do not have a unifying policy statement on access to family planning regardless of age. Therefore, Zambia is placed in the gray category for this indicator.
The
Gender Equity and Equality Act, 2015
declares that women have the right to adequate sexual and reproductive health services, including the right to access FP services and choose an appropriate method of contraception. It further elaborates that health care workers must:
(a) respect the sexual and reproductive health rights of every person without discrimination;
(b) respect the dignity and integrity of every person accessing sexual and reproductive health services;
(c) provide family planning services to any person demanding the services, irrespective of marital status or whether that person is accompanied or not accompanied by a spouse;
Because the law supports access to FP services regardless of marital status, Zambia is placed in the green category for this indicator.
The
Zambia Family Planning Guidelines and Protocols, 2006
lays out service delivery requirements for quality of care in family planning. Among the basic principles of quality of care, the Guidelines and Protocols note, is providing and ensuring a broad range of FP methods:
Choice of Methods
All women, men, and young people shall be provided with the FP methods they request, subject to them meeting the agreed eligibility criteria, without the interference of personal opinions or preconceived biases of the service providers.
The Guidelines and Protocols include a section that details each FP method currently available in Zambia, along with their mechanisms, advantages and disadvantages, side effects, service provision, and eligibility. While the eligibility criteria are derived from the World Health Organization medical eligibility criteria for contraceptive use, the Guidelines and Protocols were published in 2006 and therefore rely on outdated criteria. Even so, young people are not specifically forbidden from using any method. While some methods have no restrictions on youth based on age (i.e., progesterone only pills, injections, and implants have no restrictions for those over age 16; intrauterine devices have no restrictions for those over 20), younger individuals can use those methods with precautions.
As Zambia
s FP guidelines do not have a clear policy statement that requires health providers to offer short-acting and LARC methods, Zambia is placed in the yellow category for this indictor.
Although emergency contraception (EC) eligibility is not factored into this indicator
s rating, the Guidelines and Protocols state that while no age restrictions are listed for EC eligibility, EC should only be used in the case of rape or for clients with a history of ectopic pregnancy and other cardiovascular and chronic conditions.
The
Zambia Family Planning Guidelines and Protocols, 2006
include provision of sexual and reproductive health (SRH) information to youth as one of its key strategies to integrate family planning into adolescent reproductive health:
Provide information, education, and skills training to enable young people to deal with their RH decisions in a mature way. Do this in a variety of locations, including health services, schools, clubs, recreation centres and employment-based services.
The Guidelines and Protocols continue to stress the importance of strengthening adolescent education on reproductive health in schools:
Strengthen family education, for example. understanding of the physiology of RH system and how it works, responsible parenthood. the importance of building relationships and maintaining human values and dangers and risks associated with early sexual activities in all schools. Such information will need to be completed by appropriate service for students of reproductive age.
In 2013, the Ministry of Education and Curriculum Development Center reviewed the existing school curriculum and eventually passed the
Comprehensive Sexuality Education Framework, 2014,
which organizes the curriculum by six themes: relationships; values, attitudes, and skills; culture, society, and human rights; human development; sexual behavior; and sexual and reproductive health. The curriculum breaks down the topics, content, and outcomes for each theme along every grade level from grades 5 through 12 and includes all nine of the essential United Nations Population Fund (UNFPA) components of comprehensive sexuality education (CSE). While the curriculum encourages and discusses abstinence as a pregnancy-prevention mechanism throughout, SRH content includes contraceptives as an effective method of preventing unintended pregnancies starting in grade 9.
For example, the CSE program includes an integrated focus on gender that evolves from learning about the role of gender in society in grade 5 to the impact of gender norms on FP in grade 12:
GRADE 5
3. Culture, Society, and Human Rights
5.3.3 Social Construction of Gender
5.3.3.1 Gender Roles
Specific Outcomes:
5.3.3.1.1 Identify roles that have traditionally been assigned to males and females in society.
5.3.3.1.2 Discuss the effects of promoting gender roles.
Knowledge:
- Gender roles for females: household chores, nurturing, empathetic, emotional, childcare, elder care
- Gender roles for males: Breadwinners, leaders, protectors, initiators
- Effects of promoting gender roles: overworking of other family
members, low productivity in the home
Skills:
Critical thinking about the gender roles
Values:
Appreciation of sharing gender roles equitably
GRADE 12
5. Culture, Society, and Human Rights
5.3.3 Social Construction of Gender
5.3.3.1 Gender Roles
Specific Outcomes:
12.3.3.1.1 Explain gender equality in sexual behavior and family planning
Knowledge:
Gender equality in sexual behavior and family planning: when to have babies, collective agreements, family size, when to have sex, openness to partner
Skills: Effective
communication
about gender
equality in sexual behavior and family planning
Values:
- Appreciation of gender equality
in sexual
behavior and
family planning
- Assertiveness on gender equality
on sex
The CSE program also includes components on improving communication skills and decision-making in SRH. In addition to specific decision-making skills identified throughout each of the six components, decision-making is a topic in the second theme of
Values, Attitudes and Skills.
The curriculum notes that it is designed to expose potential risks to young people so that they can make informed decisions. It also explains that the curriculum is meant to be delivered in a safe and healthy learning environment:
The teachers shall ensure that all the outcomes covered here are shared with the learners so that while in school and out of school later, the learners will feel safe in life to face sexuality issues as individuals and severally too. What is expected in here is that teachers should be counselors of the clients in their hands, the learners. The teaching approaches should be highly learner-centered. Since the information is in core subjects to be taken by every learner; through natural sciences and social sciences, teachers are requested to find joy in noticing that as a result of this Comprehensive Sexuality Education Framework, learners will be in a better position to make informed decisions on issues relating to sexuality.
Newer health policy documents, including the
Adolescent Health Strategy, 2017-2021,
discuss the importance of continuing to scale-up CSE for adolescents in and out of school as a strategy to increase their awareness and utilization of health services.
Zambia has a strong policy environment for CSE, including reference to all nine UNFPA essential components of CSE, and is placed in the green category for this indicator.
The
Zambia Family Planning Guidelines and Protocols, 2006
note the importance of supportive behaviors over judgement when incorporating family planning into adolescent reproductive health programs:
Encourage of all people in contact with adolescents to have a supportive attitude toward them, instead of sanctions and negative reinforcement.
The Guidelines and Protocols also lay out service delivery requirements for quality of care in family planning. Among the basic principles of quality of care is providing convenient and accessible services that meet clients
needs. The Guidelines and Protocols ensure privacy and confidentiality of clients seeking FP services, although outside of referencing separate service hours, it does not specifically reference youth:
In order to ensure privacy, FP service provider should observe the following measures:
- Inform the client in advance if a physical exam is going to be undertaken. Ensure that he/she is comfortable with this.
- Make every effort to ensure privacy, for example, by rearranging furniture, if there are no separate rooms to use for examinations.
- Ask client to undress only if necessary. Do not ask the client to undress and then leave him/her waiting for a long time.
- Provide a screen if there is no dressing room.
- Any person who does not have a role in the examination room should leave during the examination. If health staff must be present, limit their number, explain the reason for their presence and ask for the client's permission.
In order to ensure confidentiality, FP service providers must observe the following measures:
- Assure the client that any information he/she provides, or the details of services received will not be communicated to others without his/her consent. Never talk about the client in the presence of other clients. Never discuss client outside of the service delivery room. If talking to colleagues about the client, include the client in the conversation. If the client prefers to leave his/her card at the health facility, file the client's records immediately after completion. Control unauthorized access to client records.
In order to provide anonymity if required, FP service providers shall:
- Retain the clients' cards at the health facility. Arrange separate service hours for young adults, men, and couples. Offer services in workplaces or the community.
The Guidelines and Protocols also outline the content of trainings that all service providers involved in FP should receive. The content includes an
IEC [Information, Education, and Communication]/Counselling
Skill Set with content on family planning and adolescent health; a Communication Skill Set with content focused on the sensitive, unbiased, open, and interactive communication process;
and a Technical Skill Set that covers
FP technologies, procedures, requirements for care and follow-up" as well as a focus on adolescent health issues.
After assessing current gaps in family planning in Zambia, the
Integrated Family Planning Scale-Up Plan, 2013-2020
identified targeting and serving quality and accessible adolescent sexual and reproductive health information and services as one of its six strategic priorities. The Scale-Up Plan reaffirms that all family planning is free at public facilities, free at nongovernmental organization (NGO) outreach sites, and provided at low or no-cost at NGO fixed sites. To meet its strategic priorities, the Scale-Up Plan also includes activities that address adolescents and youth:
SDA4. Train current health providers in comprehensive FP with emphasis on LARCs [long-acting reversible contraceptives] . Dedicated FP providers will be recruited and trained; nurses and midwives currently working where dedicated FP providers do or will do outreach will be trained and subsequently receive mentoring by the dedicated FP providers
SDA12. Provide targeted services and education to adolescents and youth. Youth-friendly service points will be established in each district in existing government buildings such as sports complexes and administrative blocks. The rooms will be refurbished with FP materials and necessary supplies. Peer educators trained to dispense pills and condoms will staff the service points.
The
Adolescent Health Strategy, 2017-2021
details a strategy to move away from adolescent-friendly projects to adolescent-responsive health systems, and includes specific activities on financing youth health services in all facilities:
Financing: Transitions are required in the way that resources are allocated and purchasing of services is designed, so as to meet the need of adolescents. The following actions may facilitate this transition:
- removing (or at least reducing) the need for adolescents to pay for services at the time of use by maximizing the number of adolescents covered by effective prepaid pooling arrangements, with adequate subsidization of vulnerable adolescents and their families;
The
Reproductive, Maternal, Newborn, Child and Adolescent Health and Nutrition Communication and Advocacy Strategy, 2018-2021
notes that adolescents and youth face many barriers when seeking FP services, including the negative attitude of health workers toward adolescents and youth, and outlines essential actions to
provide capacity building and simple job aids to providers to facilitate counseling of adolescents on reproductive health/FP issues
and
train health providers and peer educators in counseling skills and sensitize them to adolescent perspectives and empathetic attitudes.
Finally, the
National Standards and Guidelines for Adolescent Friendly Health Services, n.d.
also include patient privacy and provider training to foster non-judgmental and respectful attitude toward adolescents as two requirements for service provision standards.
The policies reviewed clearly address the need to train and support providers to offer adolescent-friendly contraceptive services, as well as provide confidentiality and audio/visual privacy and free FP services. Zambia is placed in the green category for this indicator.
The
Gender Equity and Equality Act, 2015
declares that the Ministry of Health shall take appropriate measures to ensure that women access family planning information and services on an equal standing as men.
The
Zambia Family Planning Guidelines and Protocols, 2006
include three strategies for family planning, the first of which is to better integrate family planning with other reproductive health programs. The strategy specifically outlines activities to increase male involvement and address existing gender norms:
- Improve communication between couples about decisions regarding fertility and FP that would reflect the needs and desires of both men and women.
- Provide men with needed information that would enable them to participate responsibly in FP decision-making. They can get information and learn more about FP by accompanying their partners on clinic visits and by taking advantage of special clinic hours for men where available.
- Organize services for FP for men either through STI [sexually transmitted infection]/HIV prevention and control clinics or allocating special times in MCH [maternal and child health]/FP clinics when they could receive appropriate information and private services.
- Allow men to participate in the design and implementation of FP and RH [reproductive health] services and to express ways in which they can be encouraged to take more responsibility.
The Guidelines and Protocols' second strategy is to expand access to family planning through private delivery systems. This strategy includes information, education, and communication (IEC) activities to improve understanding of RH and FP rights and to change attitudes regarding FP/RH, but does not specifically connect the activities to community support of youth access to FP.
The
Adolescent Health Strategy, 2017-2021
details a strategy to move away from adolescent-friendly projects to adolescent-responsive health systems, and includes specific community-based activities:
Service delivery: A transition is needed from
adolescent-friendly
projects to programmes that strengthen mainstream capacity at primary and referral levels to respond to the priority health and development needs of adolescents. A number of actions would facilitate this transition:
- raising awareness about the health needs of adolescents and generating community support for the delivery of the adolescent health care package and for its uptake.
Preventive care: Transitions are required to create opportunities for all adolescents to make contact with primary care services for individual preventive services. Countries
experiences179 180 suggest that actions to facilitate this might include:
- undertaking community-based initiatives for demand creation through peers, community health workers, lay counselors and others.
The Health Strategy also identifies cultural and religious values and norms as a gap that prevents parents and communities from addressing SRH for adolescents and young people, including the promotion of contraception. It outlines two proposed interventions and activities:
Identified Gap/s
Some cultural and religious values and norms prevent parents, communities and schools from addressing HIV education and SRH&R for adolescents and young adults.
(i.e. Cultural issues
where parents do not talk to their children about sexuality and teachers are culturally constrained in teaching HIV and SRH)
Religious values and norms preventing parents, communities and schools from addressing HIV and SRH & R (i.e. assumptions that the promotion of contraceptives is promoting sex before marriage, etc.).
Proposed Intervention 1
Development and deploy an advocacy strategy targeting parents, communities, church and traditional leaders, school teachers and the adolescents
Indicative Activities [for Intervention 1]
-Develop and adopt an HIV/ASRH&R [adolescent sexual and reproductive health and rights] Programme approach to reach parents, community leaders, church leaders and school teachers on risk and vulnerabilities of adolescent girls and young women (AGYW)
- Develop and implement an innovative advocacy strategy targeting key bottlenecks and stakeholders.
-Under the national adolescent health (ADH) strategy mobilize communities, parents, teachers and adolescents on the availability of responsive health services.
- Undertake HIV and SRH awareness raising briefings for PTAs [parent-teacher associations] and faith-based organizations on social norms which inhibit adolescent girls and young women (AGYW) access to relevant HIV and SRH information and services.
- Review and revise training materials for health and school-based counsellors and social workers to ensure AGYW issues are prioritized (Utilize existing structures)
- Review the curricula for the alangizi (traditional teachers on SRH and HIV) to ensure AGYW issues are being addressed.
Proposed Intervention 2
Development of communication campaigns with innovative approaches and tools to promote AGYW health seeking behaviours and increase their knowledge on sexual health and development opportunities.
Indicative Activities [for Intervention 2]
- Launch sustained national mass and interpersonal communication campaigns on what has changed, what we can do & how we can do it.
- Information dissemination through sensitization workshops for traditional leaders (paramount chiefs, chiefs, sub chiefs, indunas, headmen
- Identify of key champions (political, traditional, civil society, youths, church leaders) to use in the change campaigns
- Develop, print and disseminate targeted HIV and SRH IEC materials (posters, brochures, leaflets, etc.) for opinion leaders, parents and different groups of AGYW (in local languages)
- Review and revise and re-develop innovative and adaptive life skills, CSE [comprehensive sexuality education] and peer education modules for use by different cadre (teachers, CBO [community-based organization] volunteers, health and youth workers, community volunteers, peer educators, etc.)
The
Reproductive, Maternal, Newborn, Child and Adolescent Health and Nutrition Communication and Advocacy Strategy, 2018-2021
acknowledges parents
discomfort around talking to their children about FP and that many community leaders embrace
cultural and traditional beliefs which impact negatively on the acceptance of modern contraceptives by women and young girls.
The Communication and Advocacy Strategy outlines multiple communication tasks and essential actions that can be taken to improve parents
comfort discussing FP with their children and reach an increased number of community leaders that support youth and adolescents seeking FP and health services.
Moreover, the
Zambia Integrated Family Planning Costed Implementation Plan and Business Case, 2021-2026" includes a sub-activity to produce standard communication materials to be used by all stakeholders for different groups, including adolescents. It also outlines other activities to create an enabling social environment for the youth:
FP coordinators to support adolescents and youth to promote FP among peers
Design and implement FP information materials and service delivery infrastructure for adolescents,...
Zambia
s policies outline specific interventions to build support within the larger community for youth FP and address gender norms. Therefore, Zambia is placed in the green category for this indicator.

{kind=link}
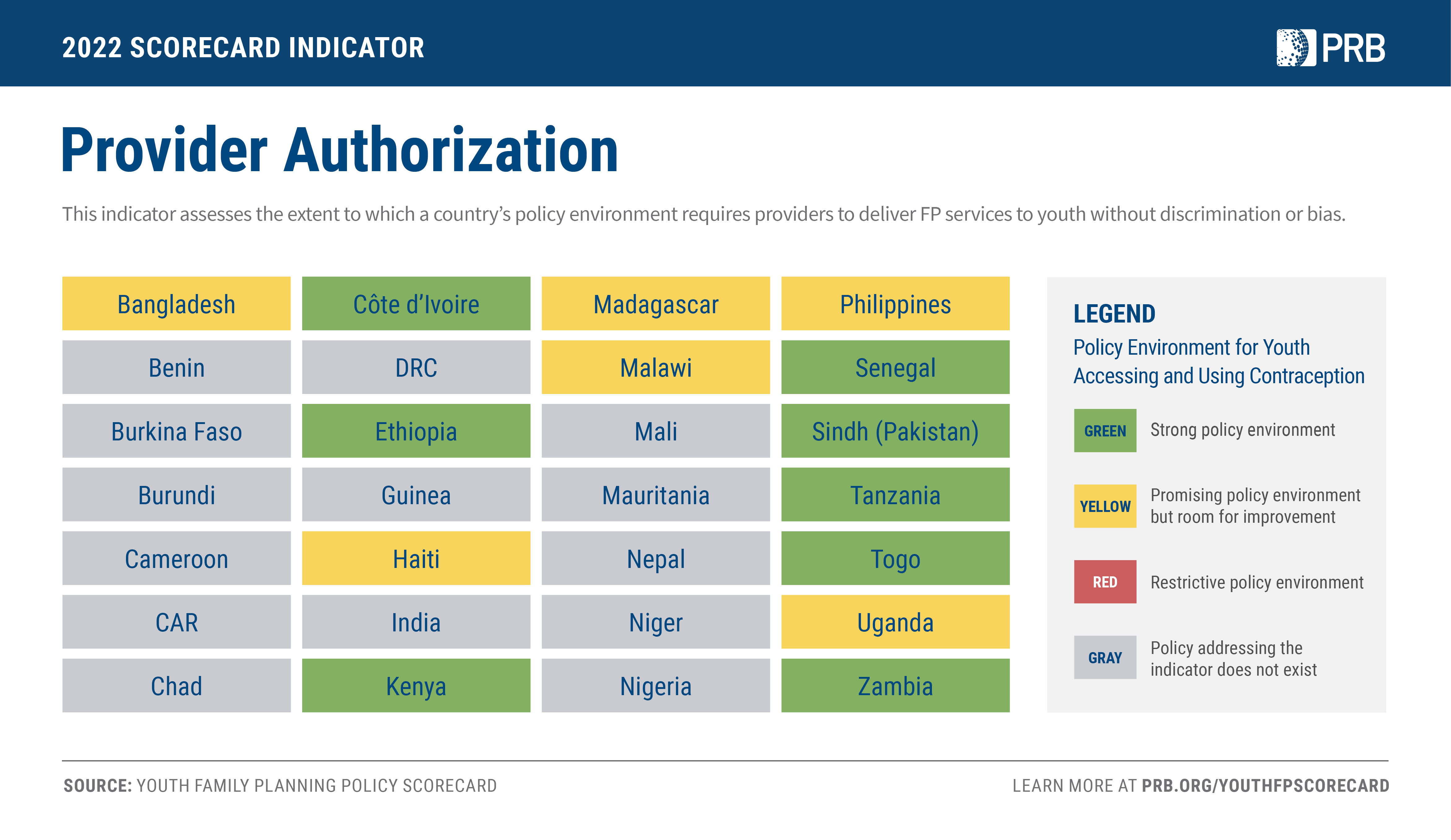{kind=link}
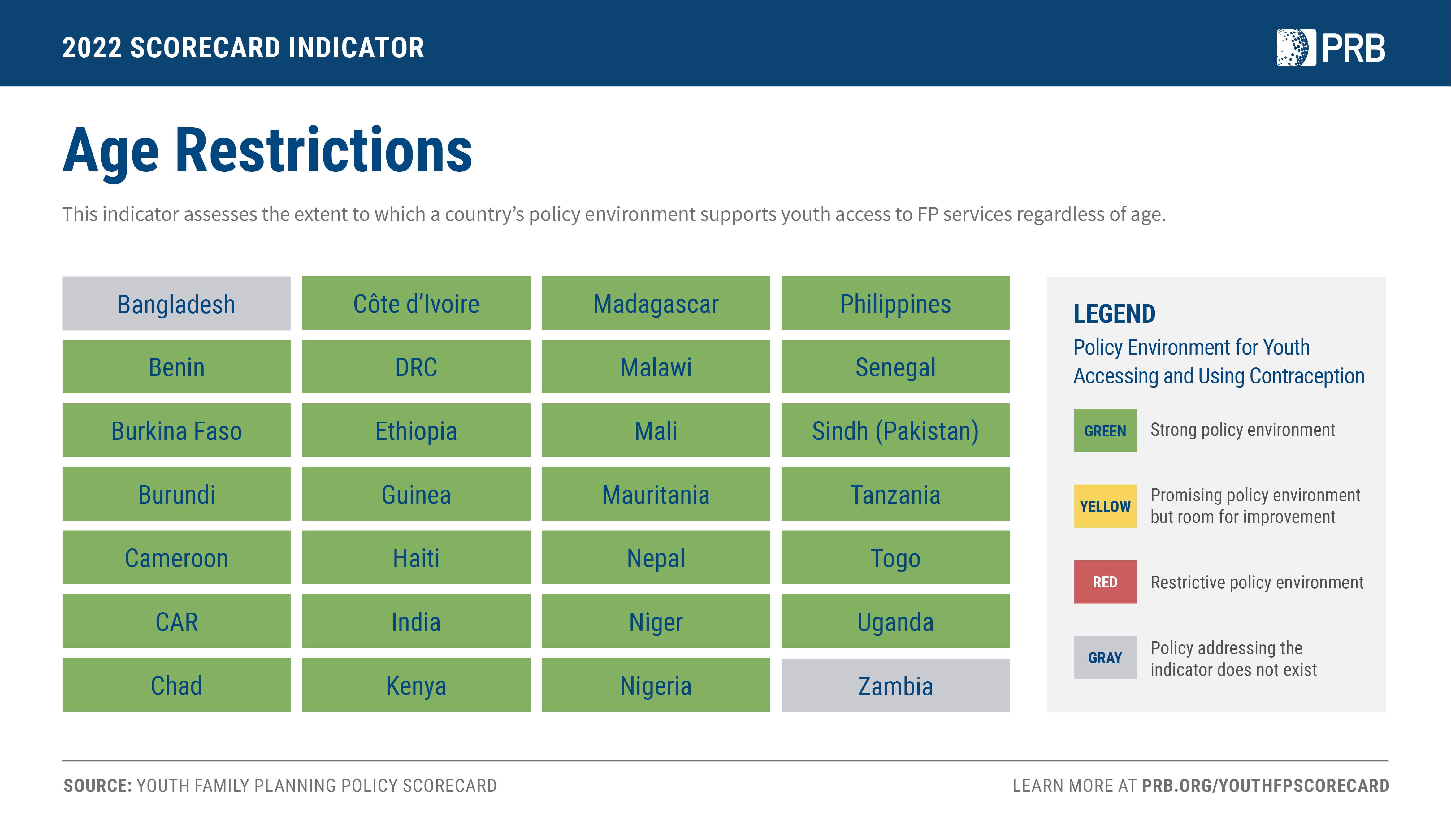{kind=link}
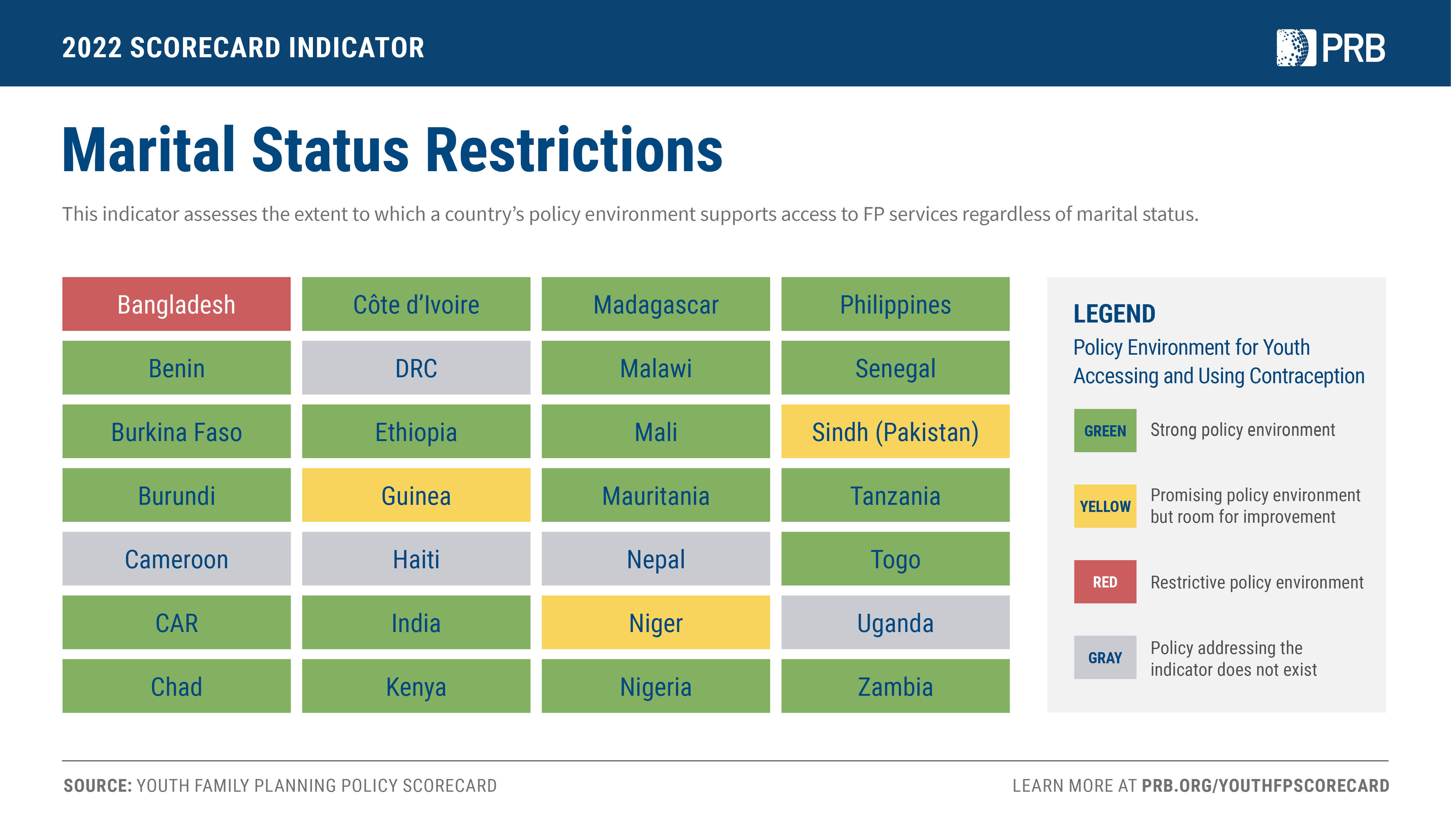{kind=link}
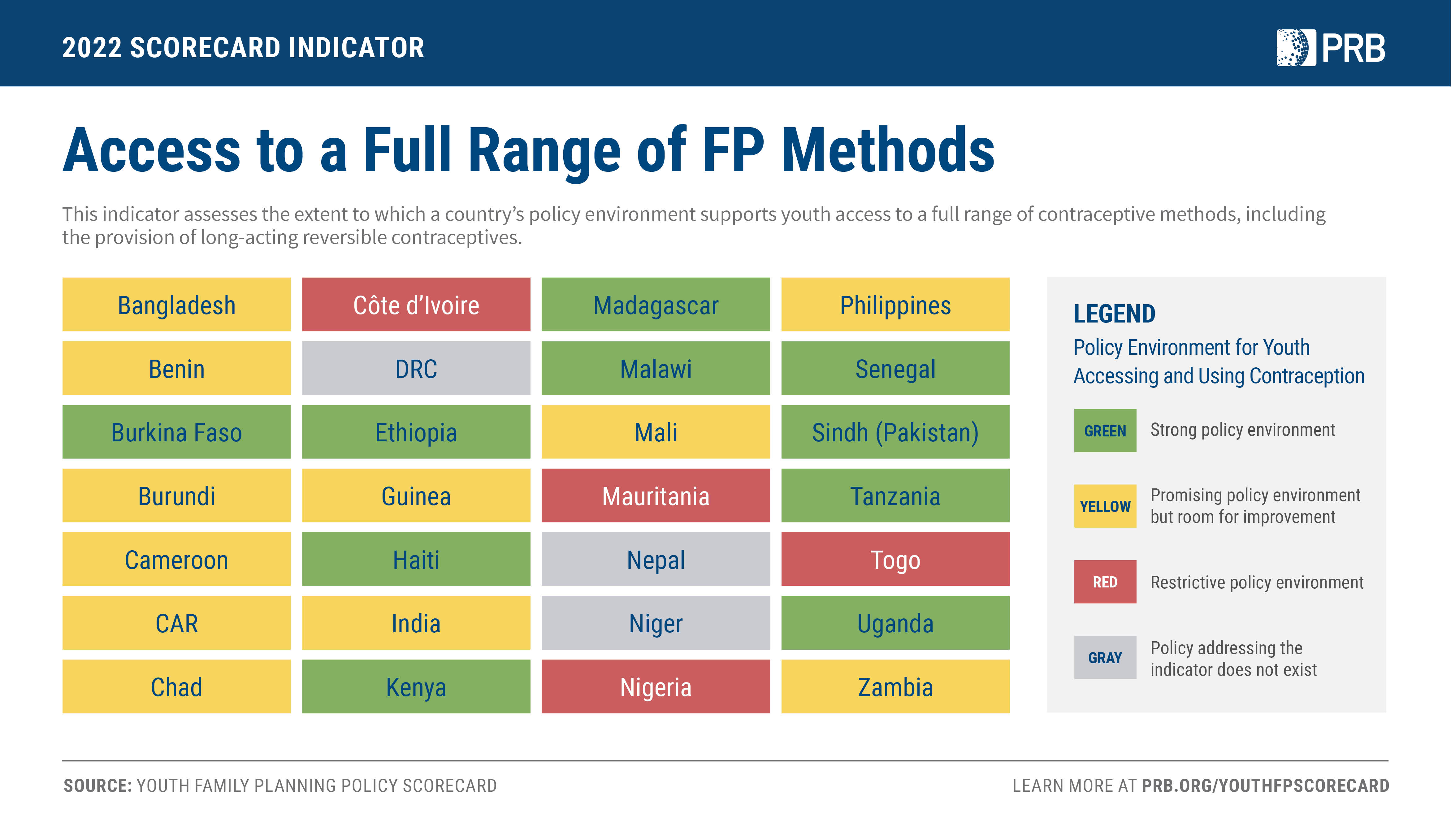{kind=link}
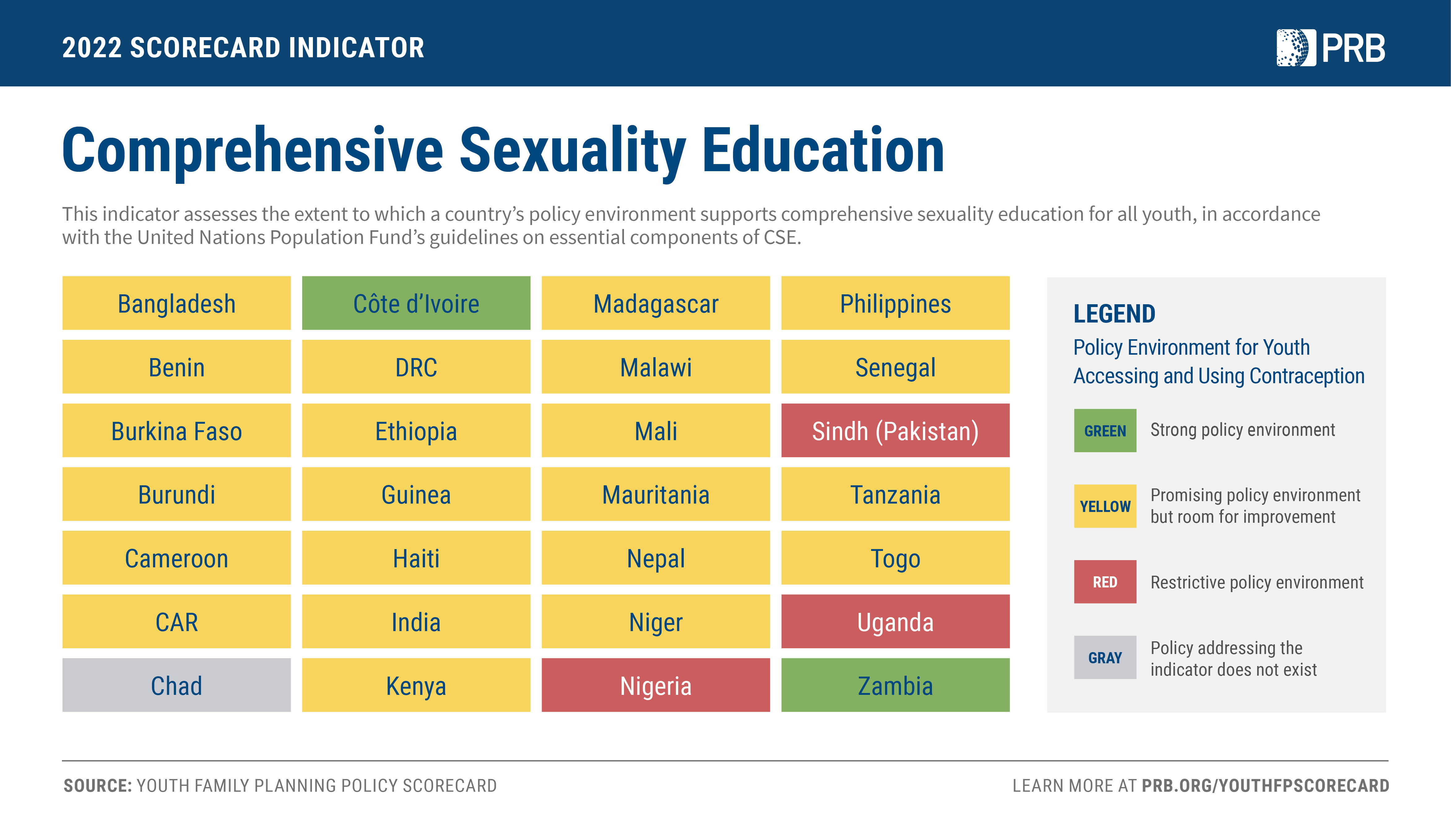{kind=link}
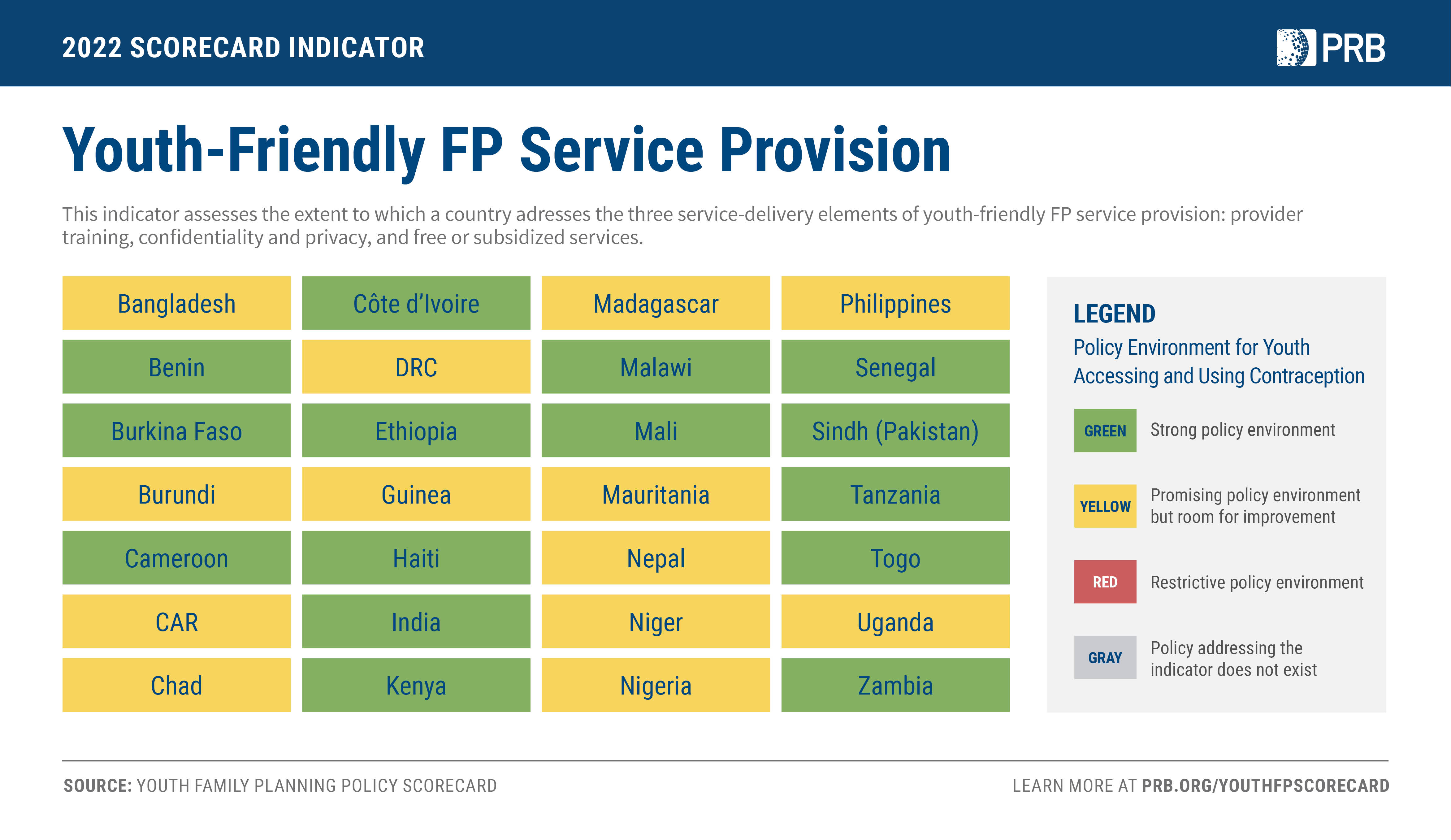{kind=link}
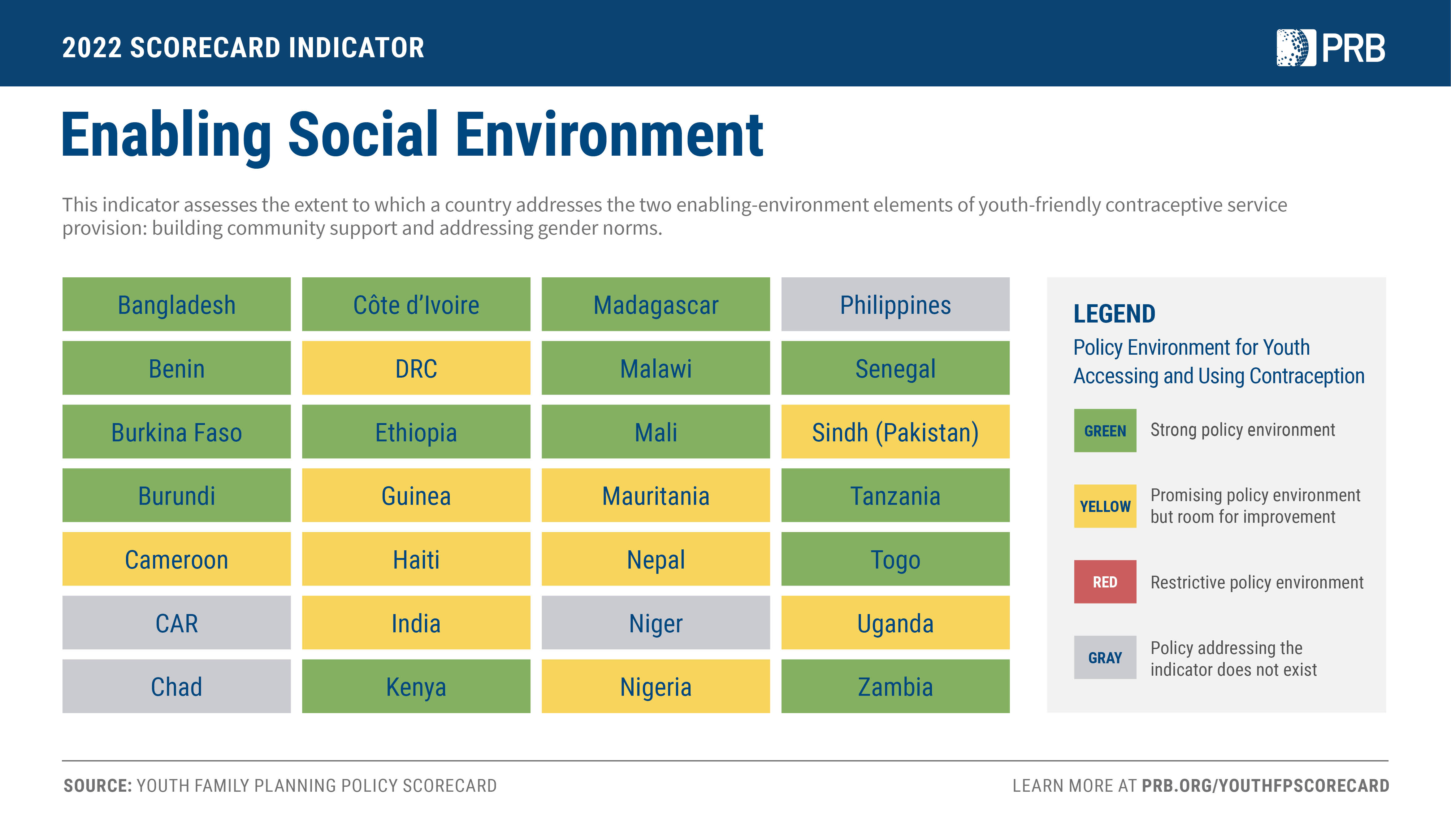{kind=link}
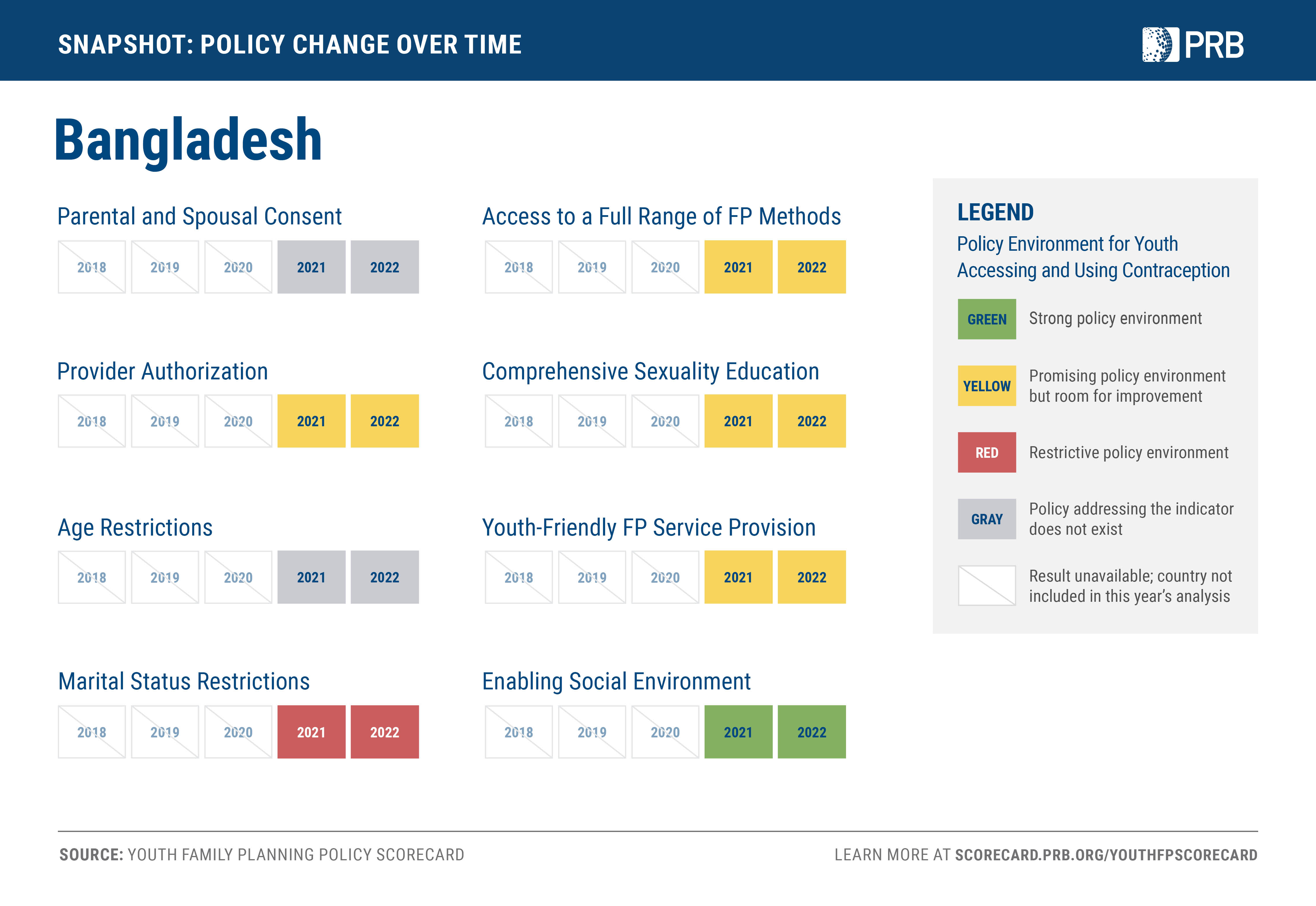{kind=link}
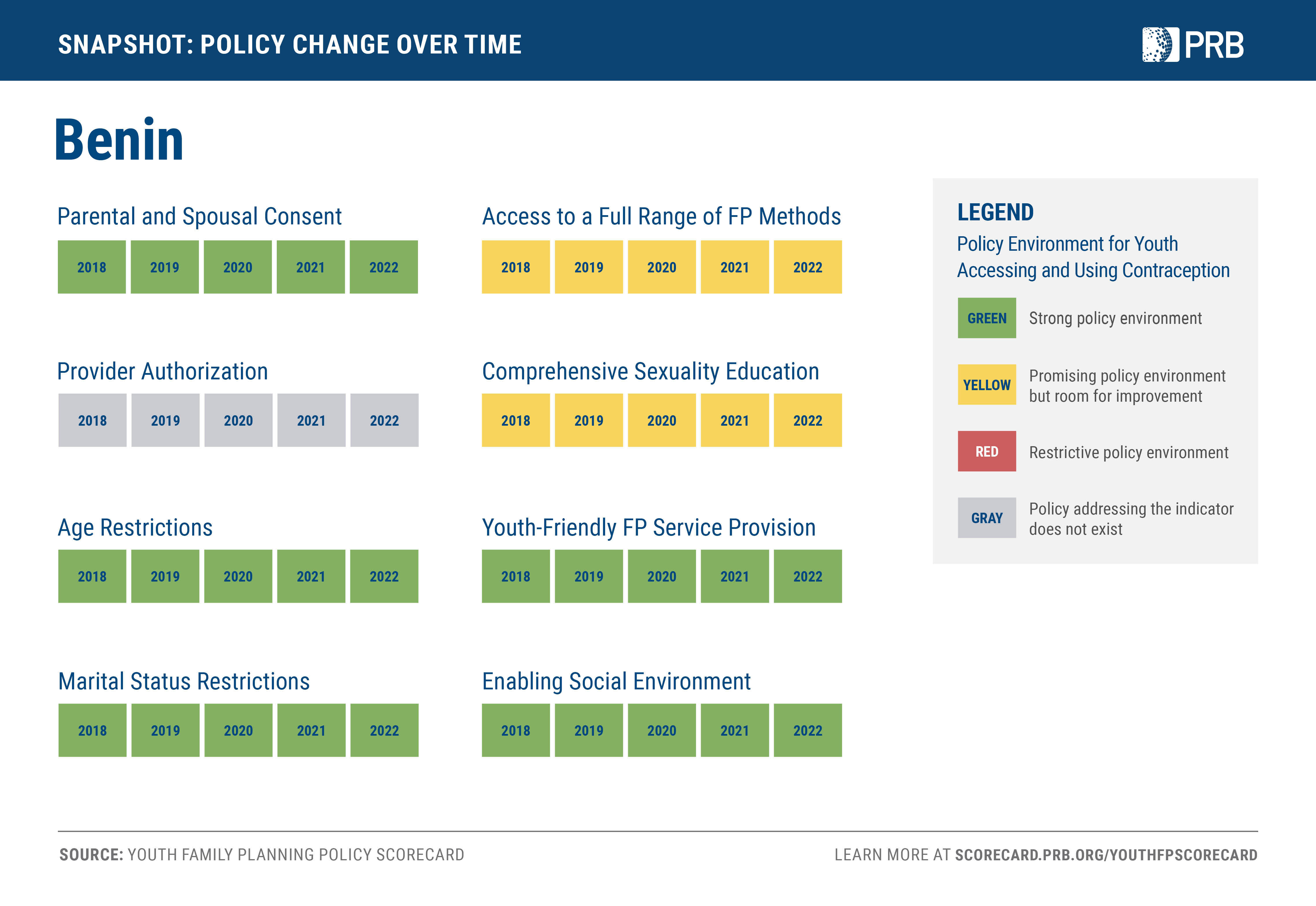{kind=link}
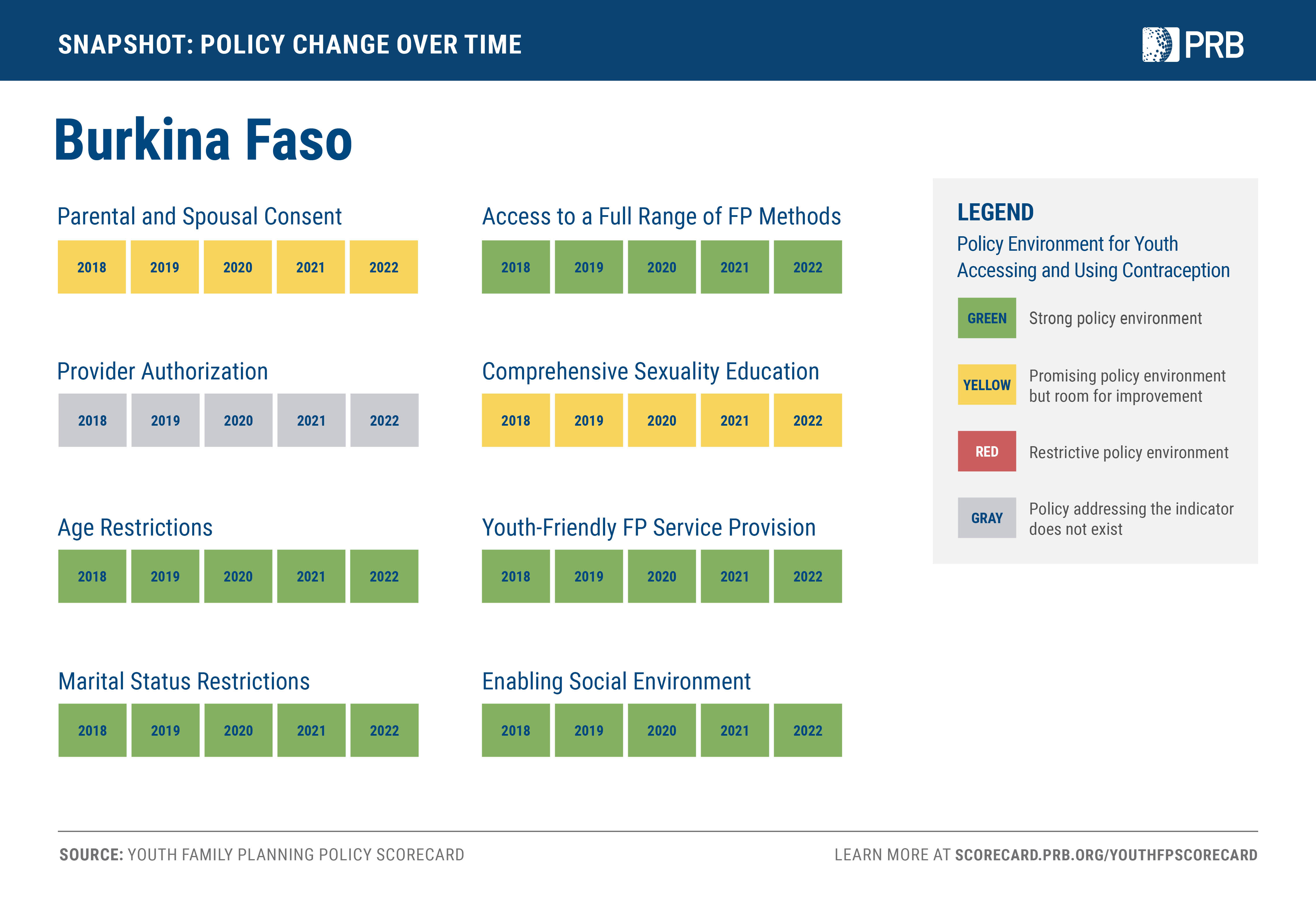{kind=link}
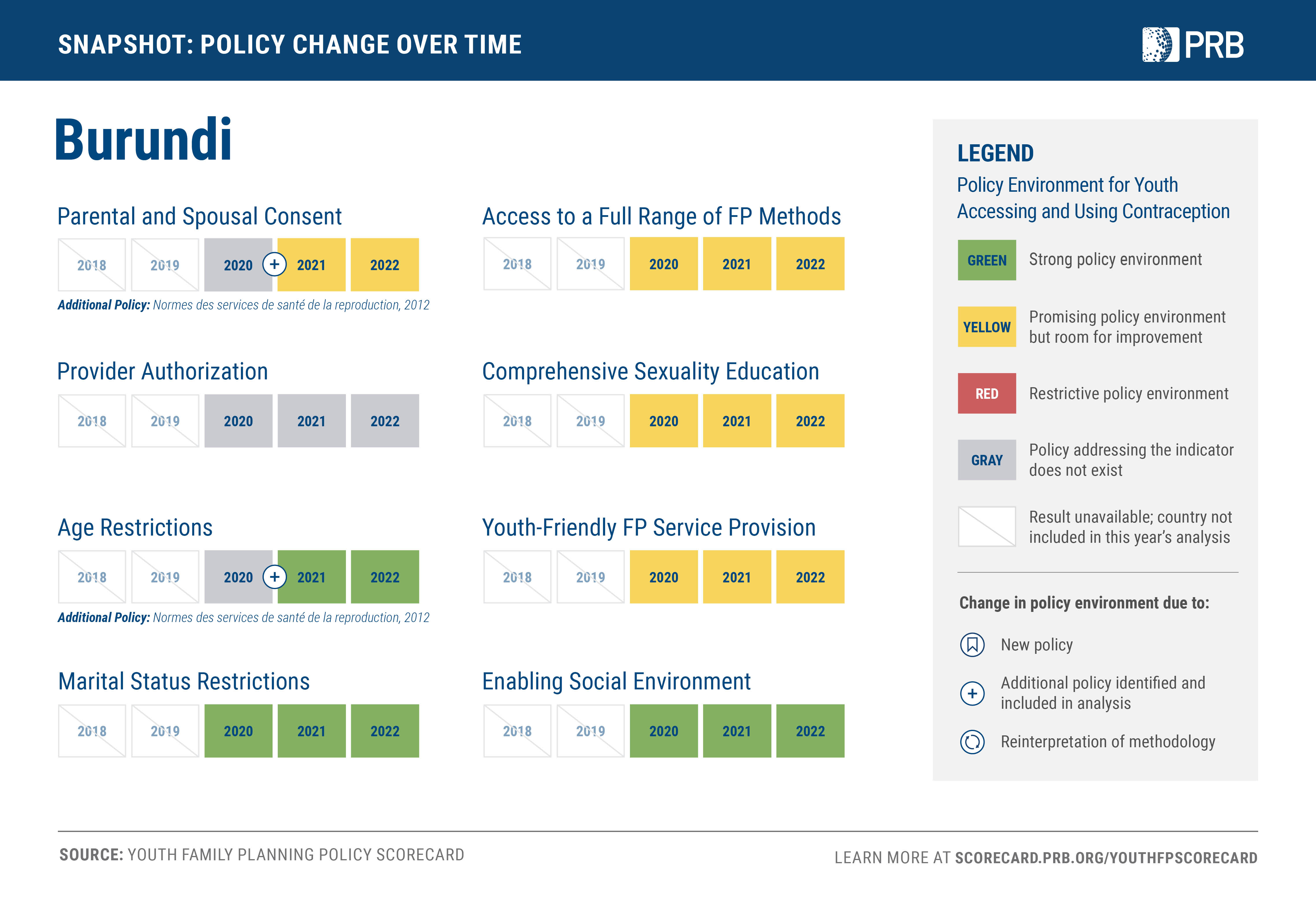{kind=link}
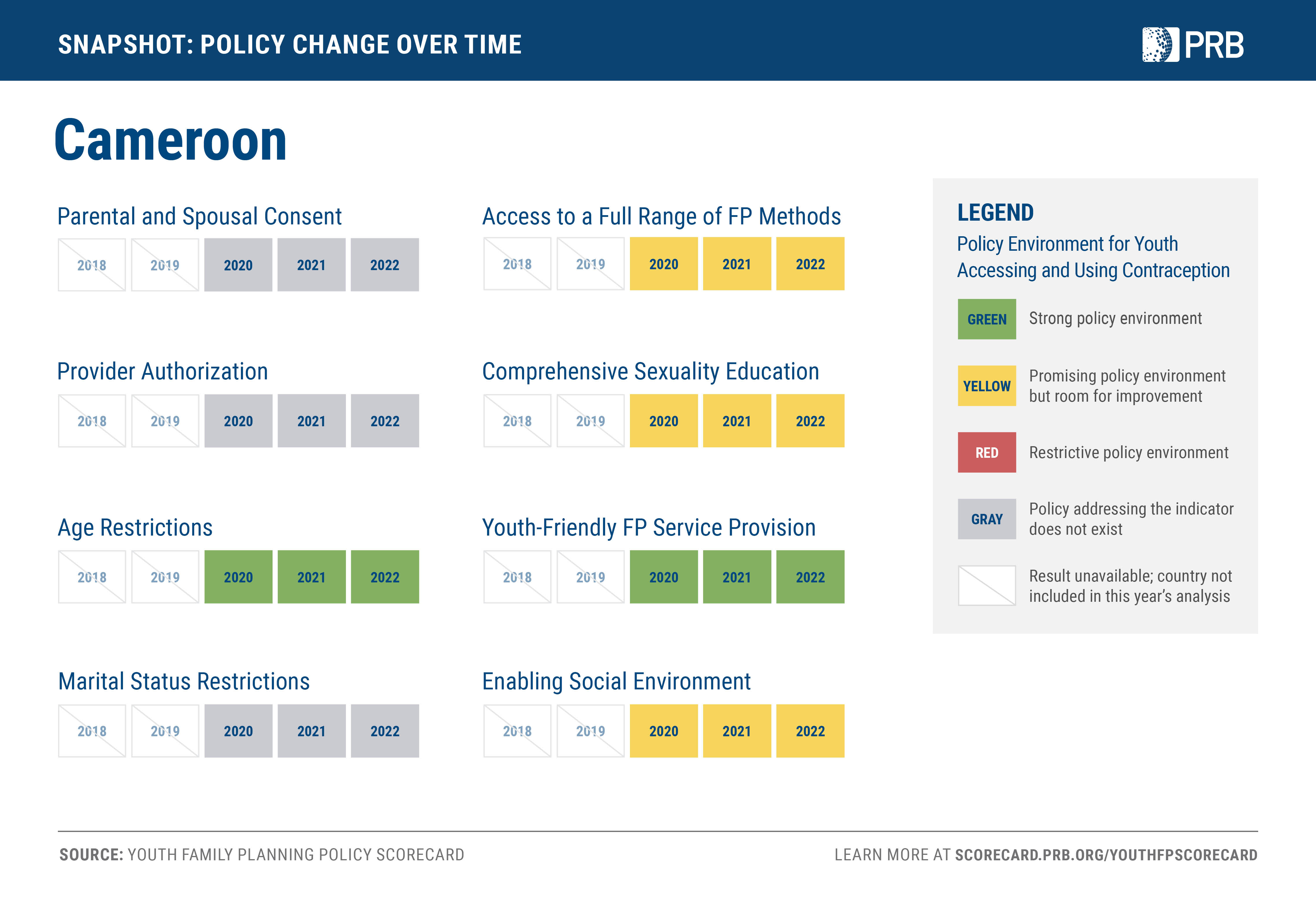{kind=link}
{kind=link}
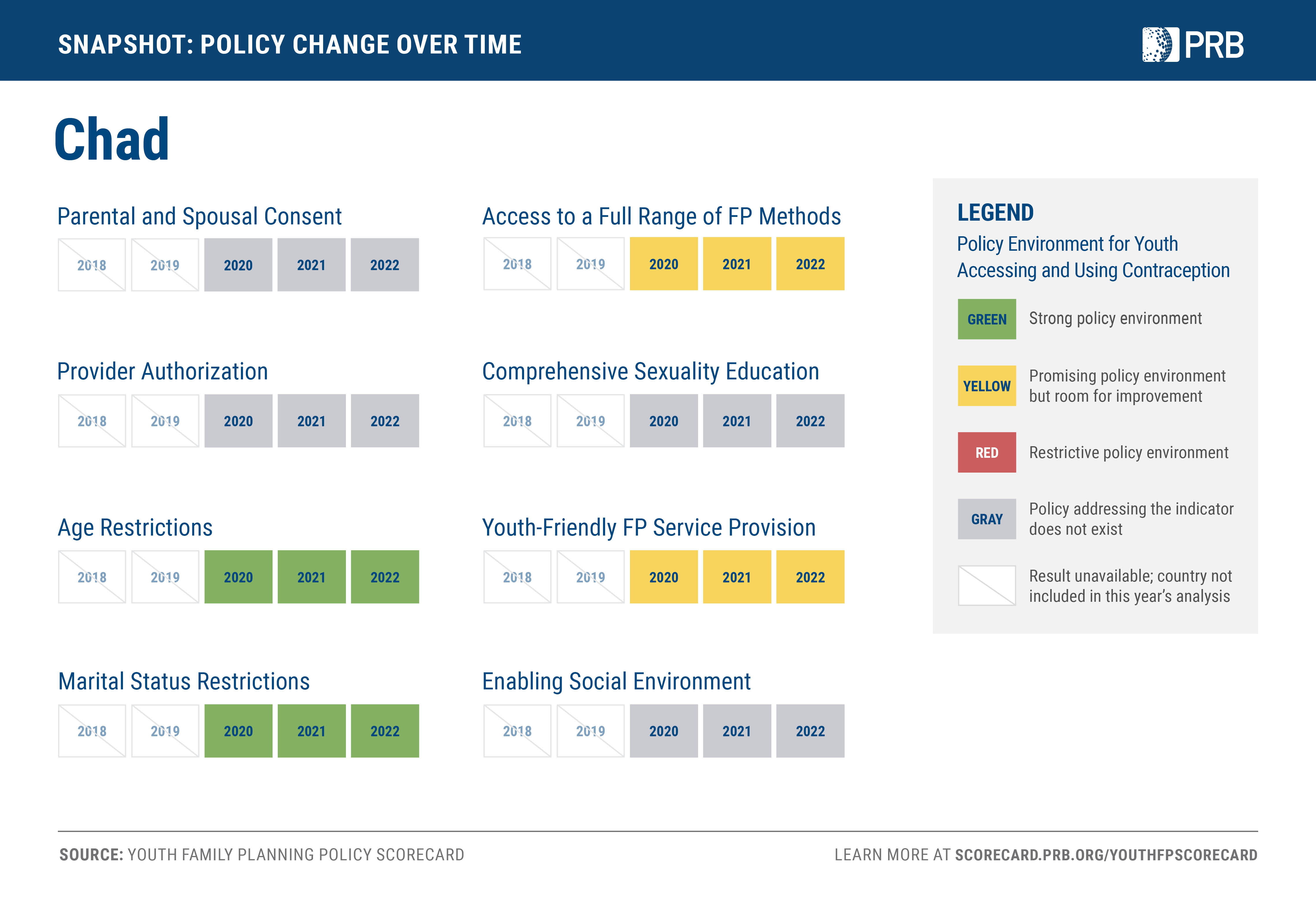{kind=link}
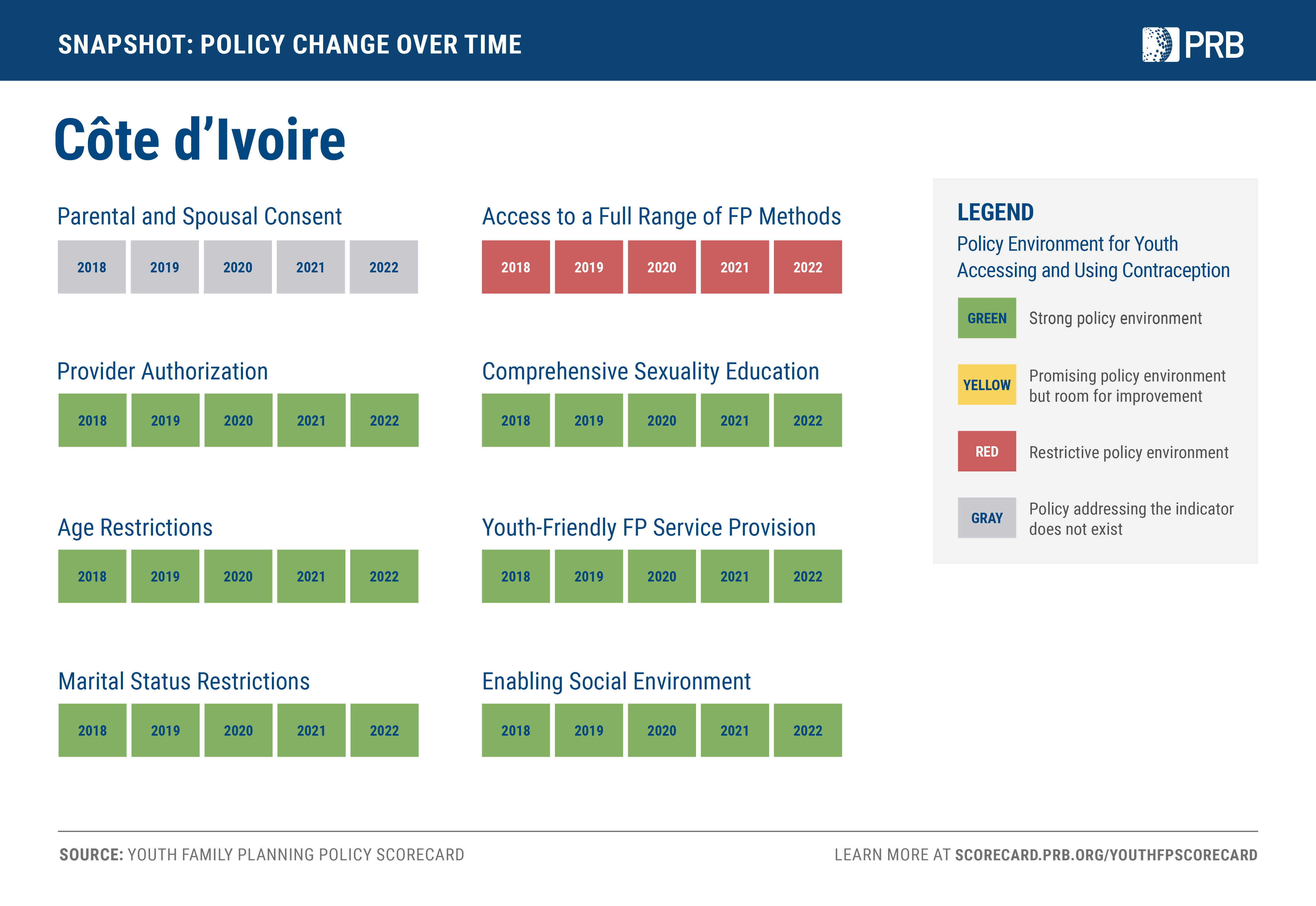{kind=link}
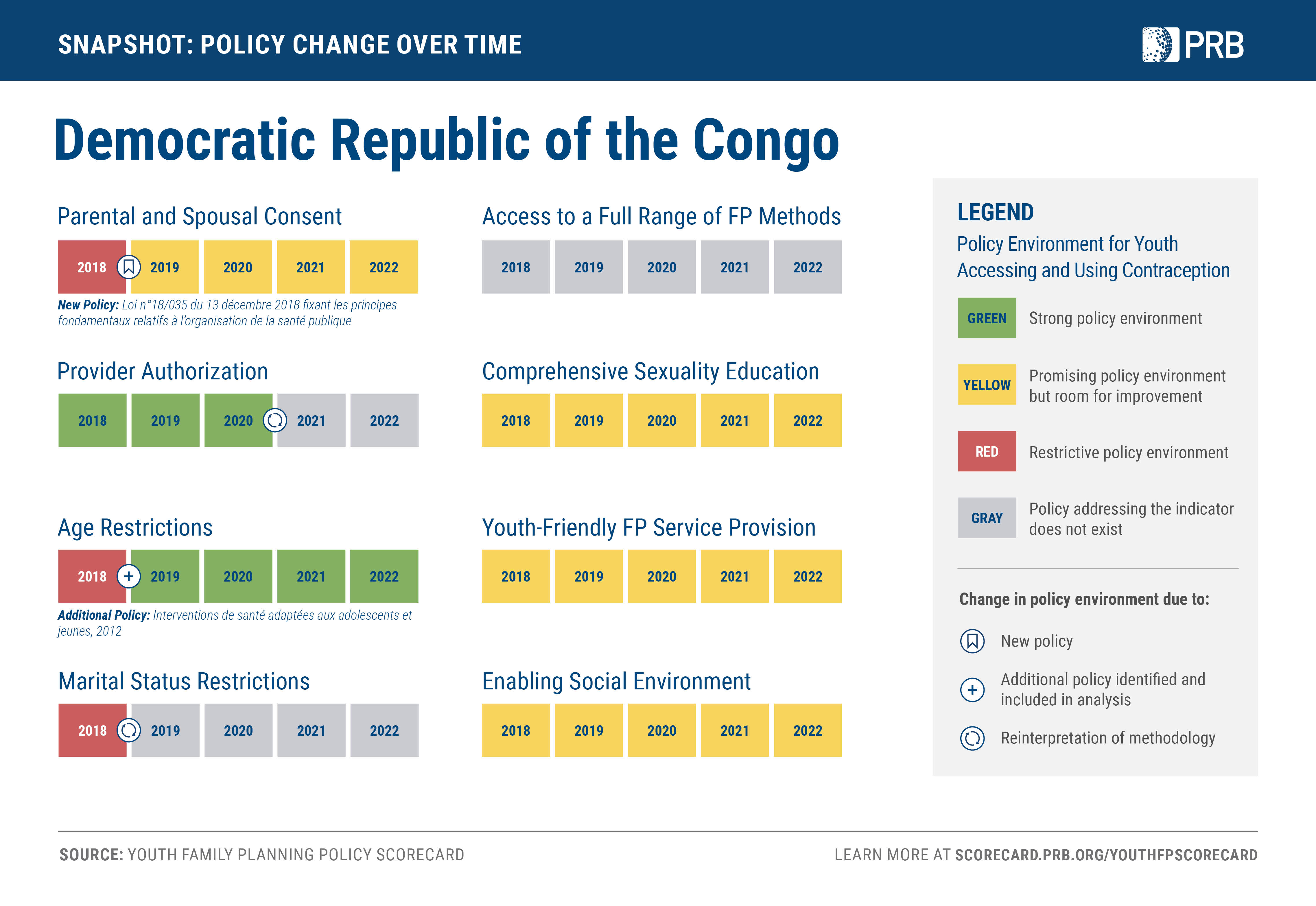{kind=link}
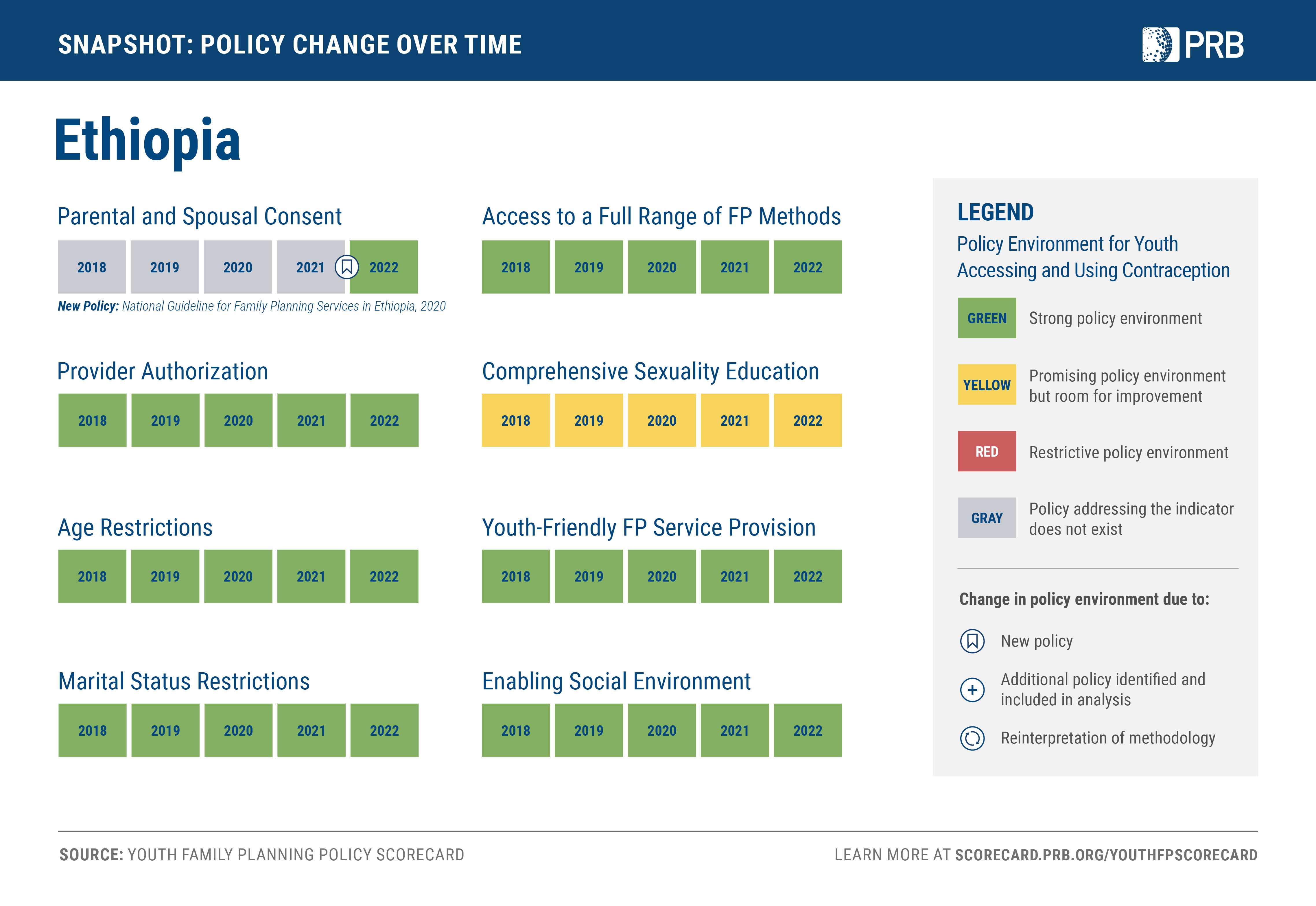{kind=link}
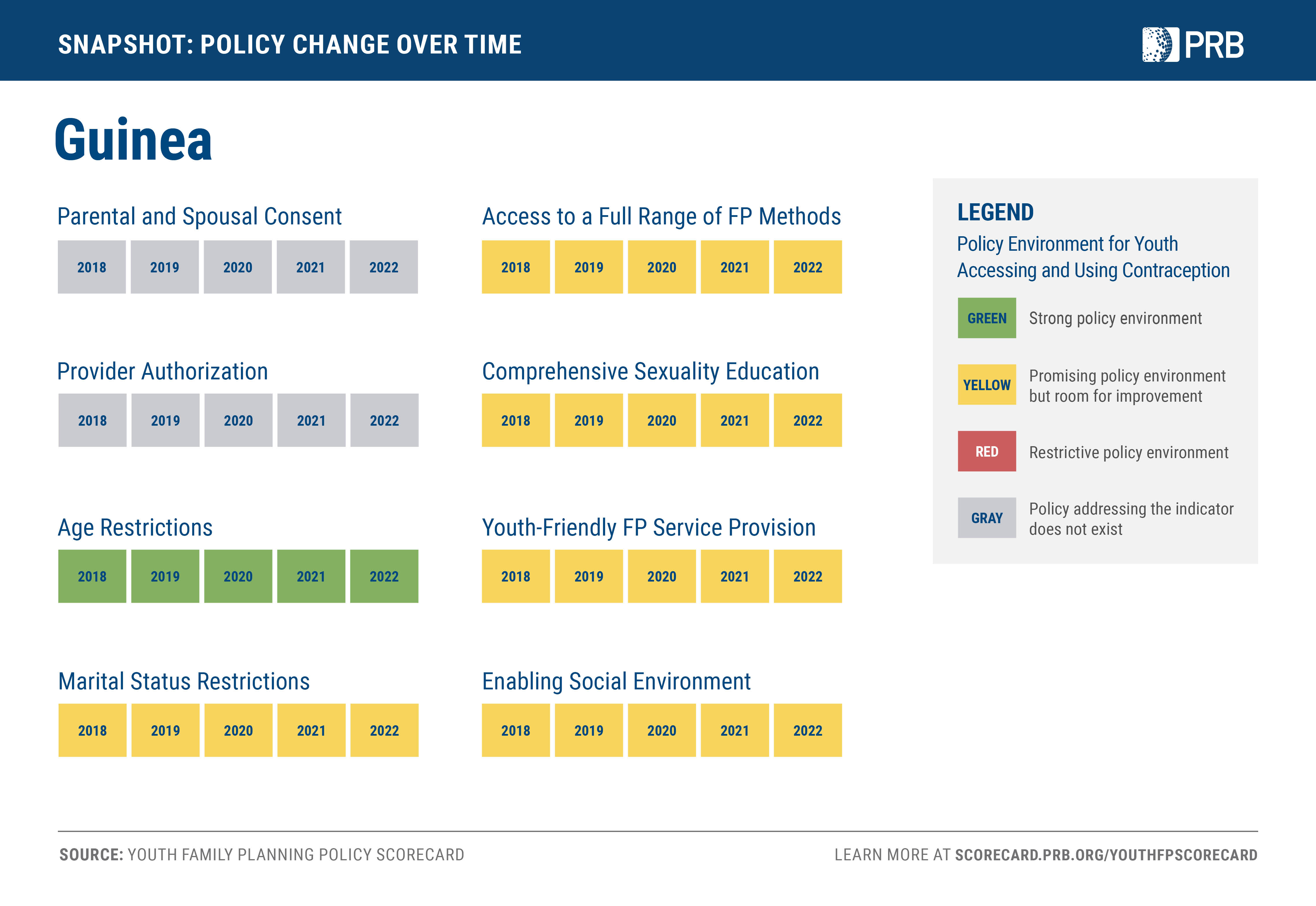{kind=link}
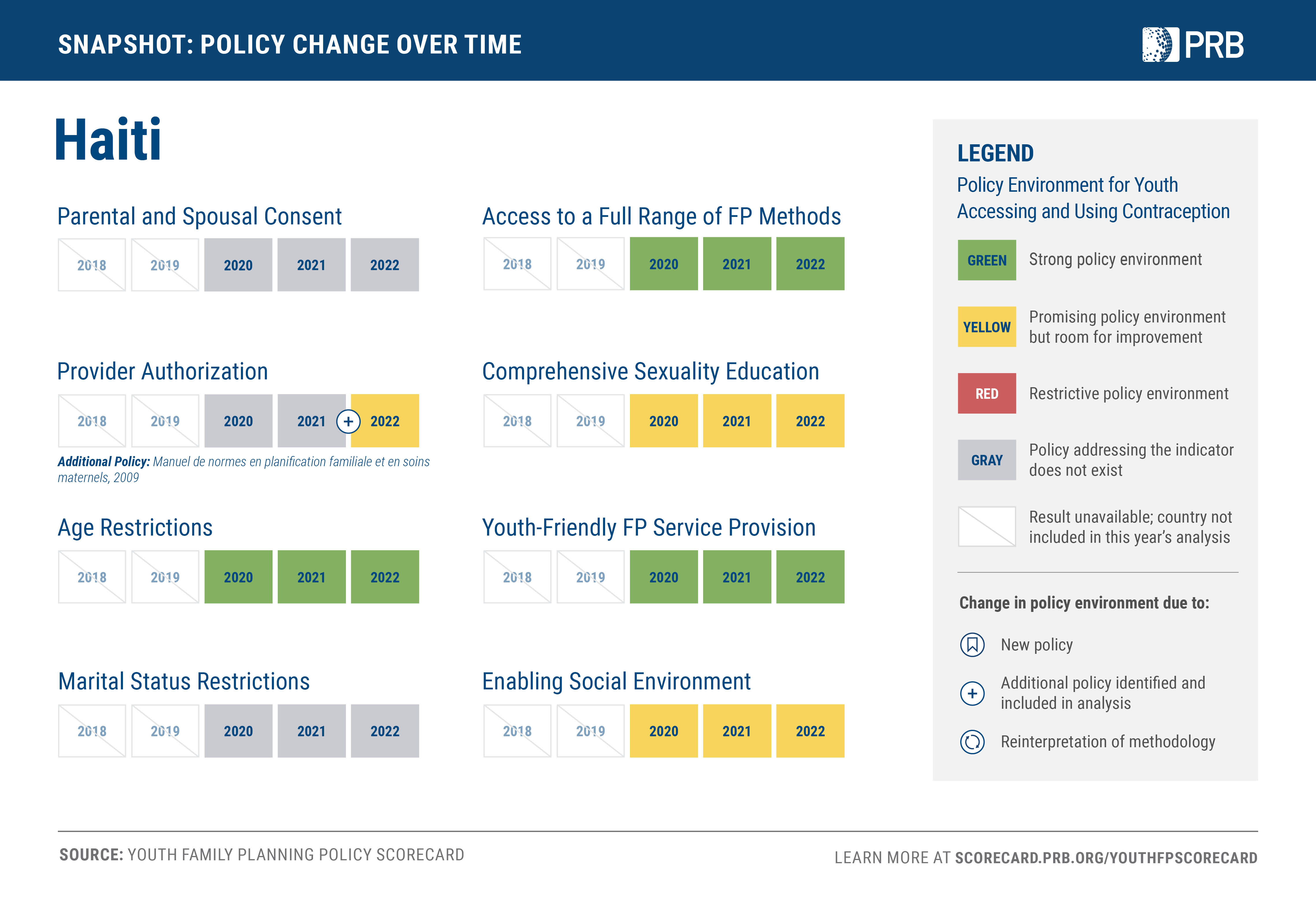{kind=link}
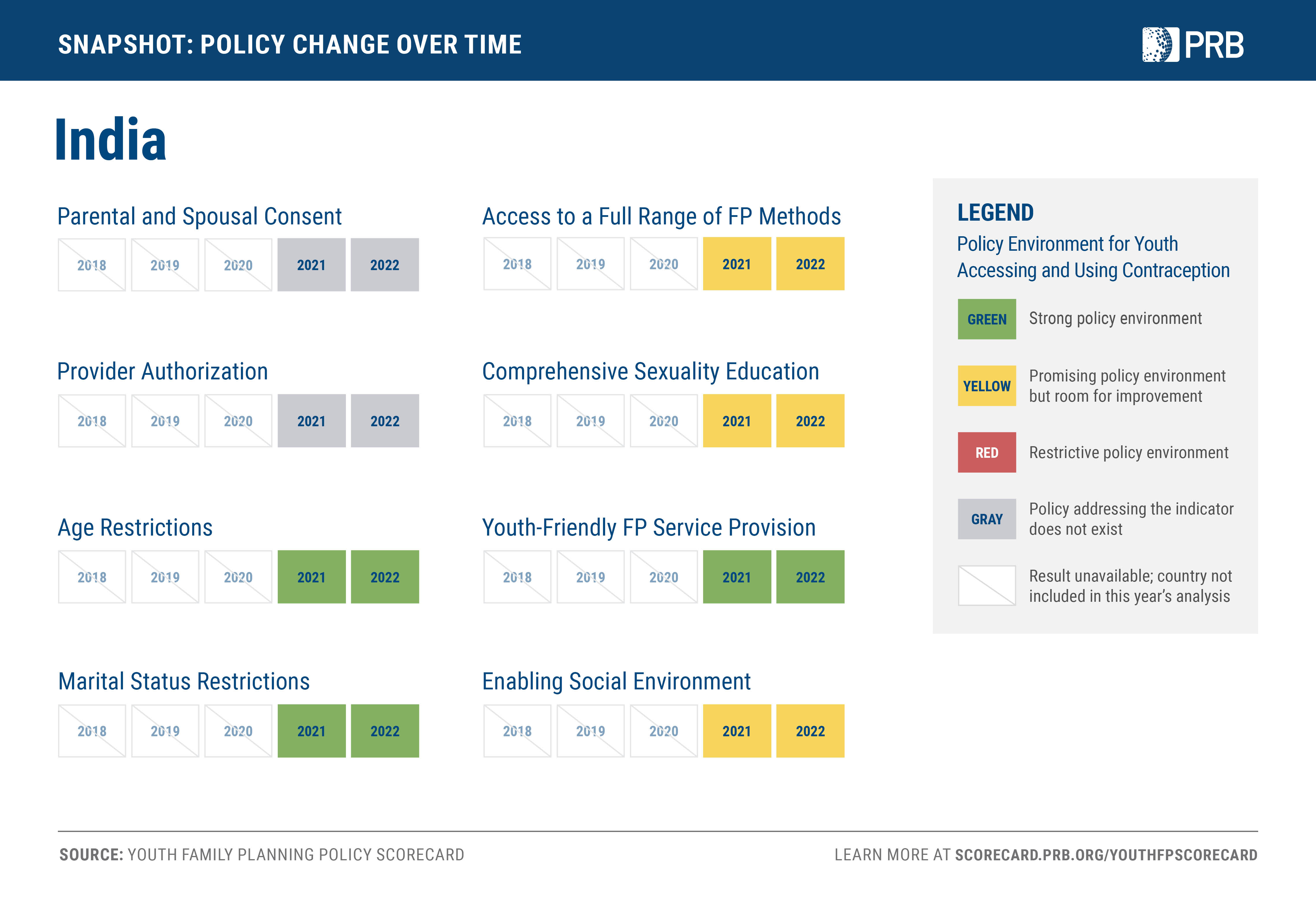{kind=link}
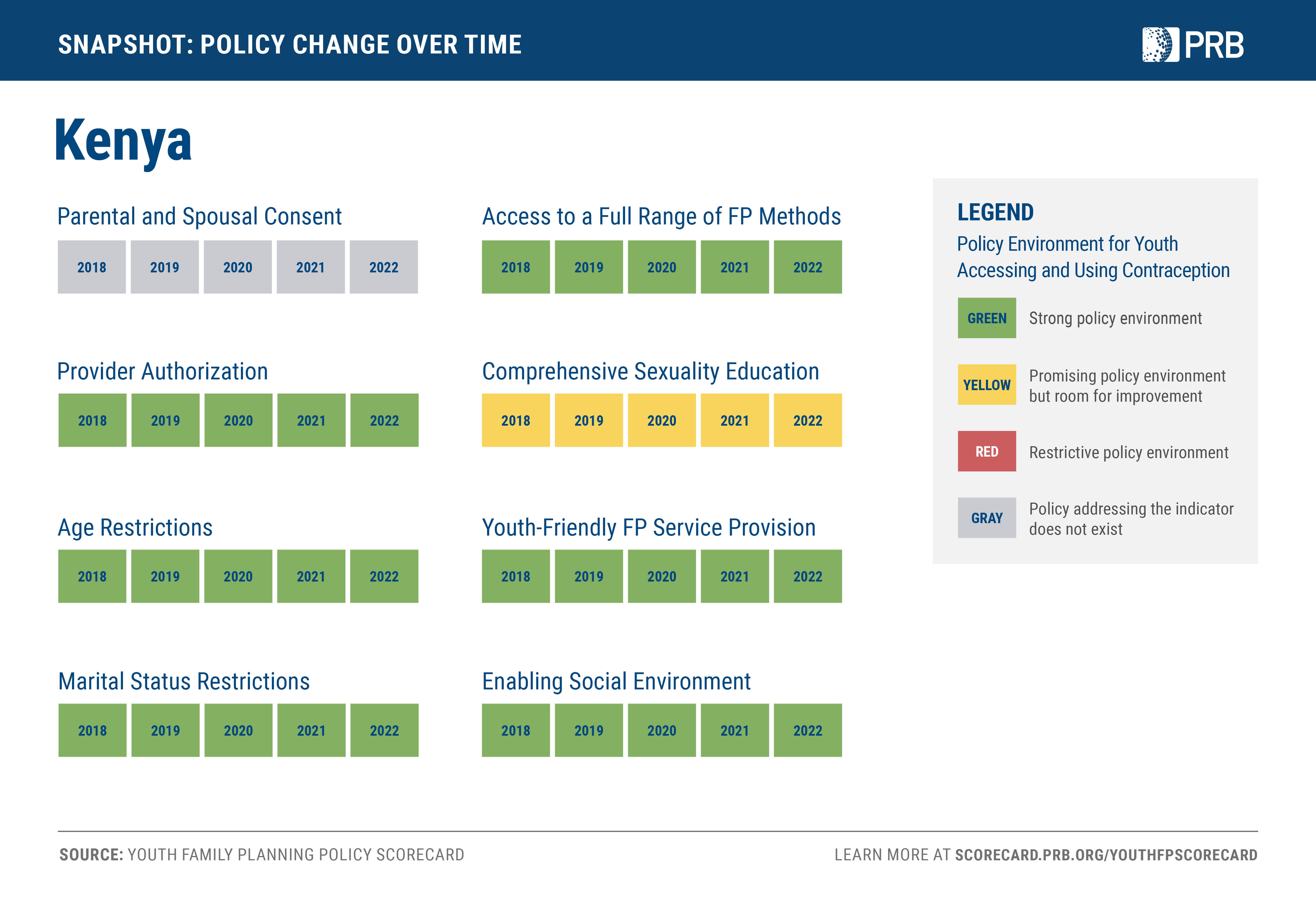{kind=link}
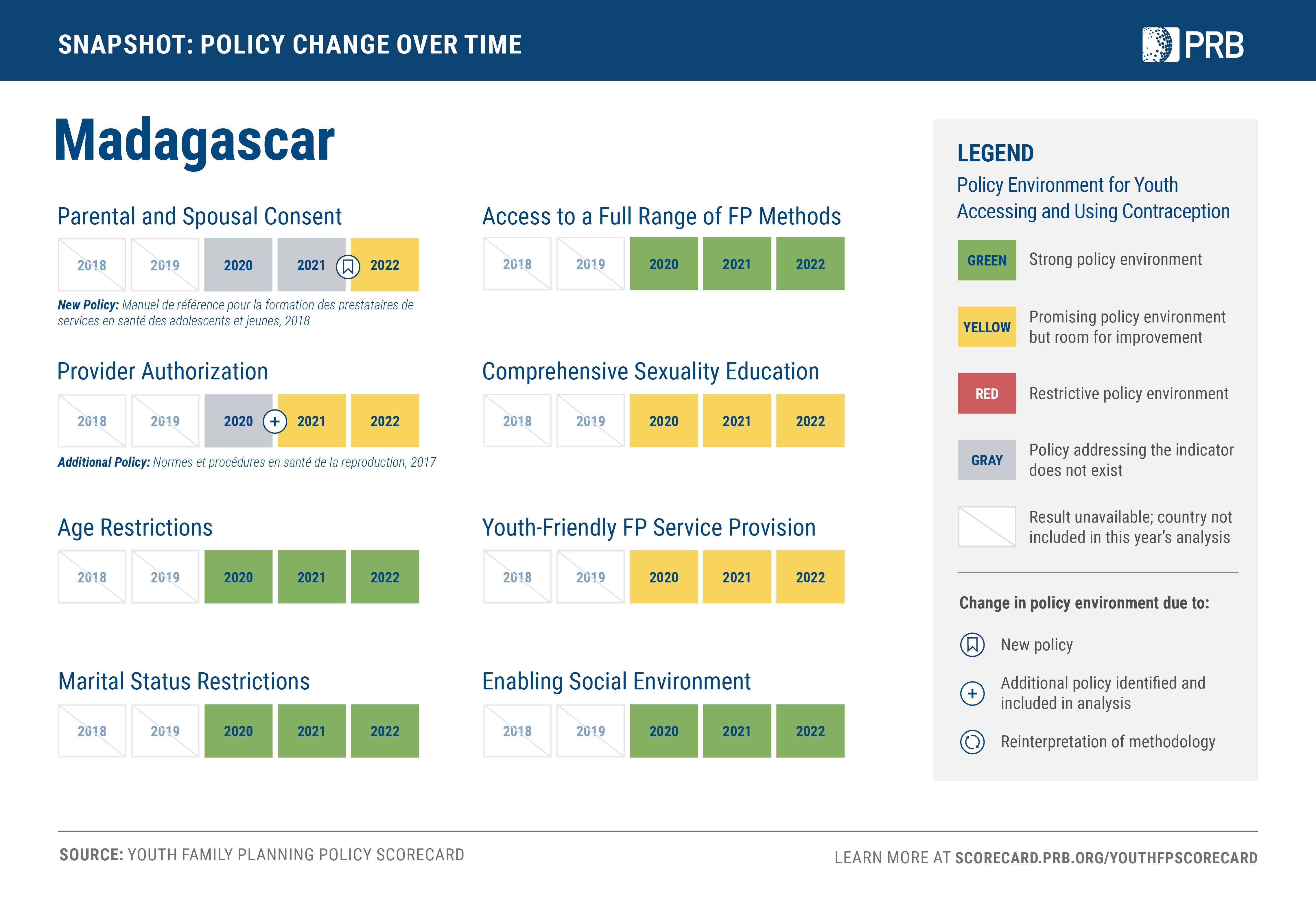{kind=link}
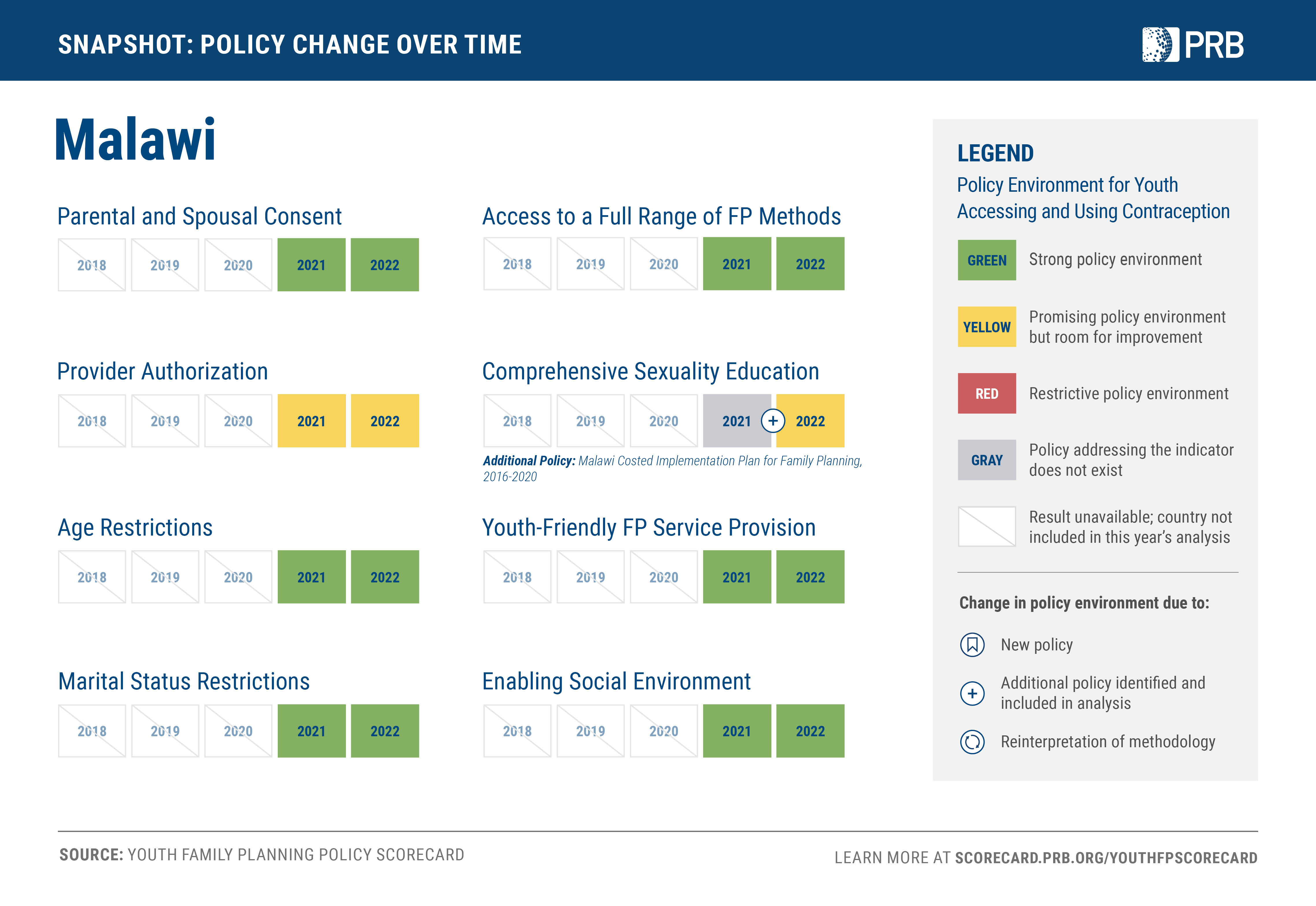{kind=link}
{kind=link}
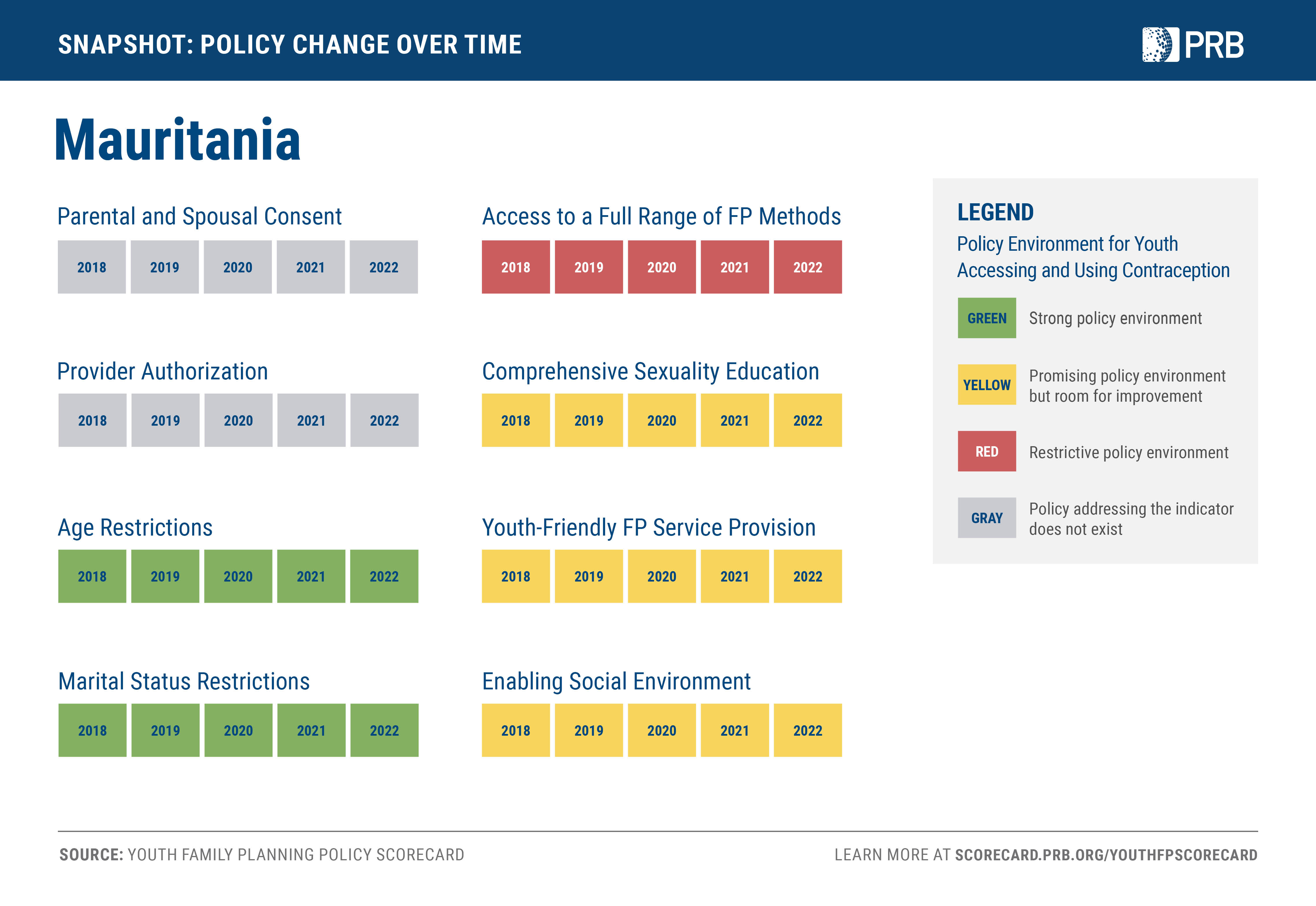{kind=link}
{kind=link}
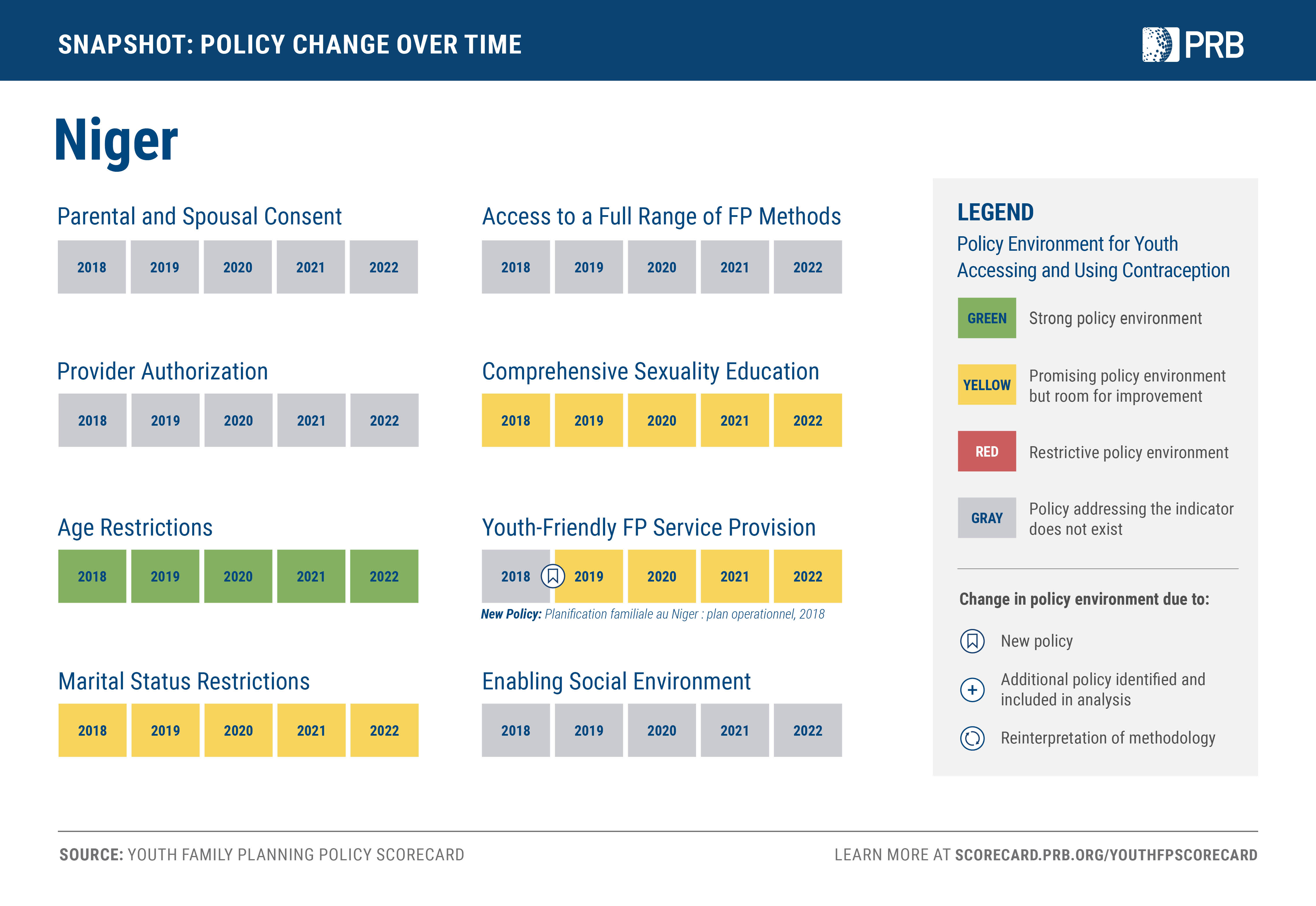{kind=link}
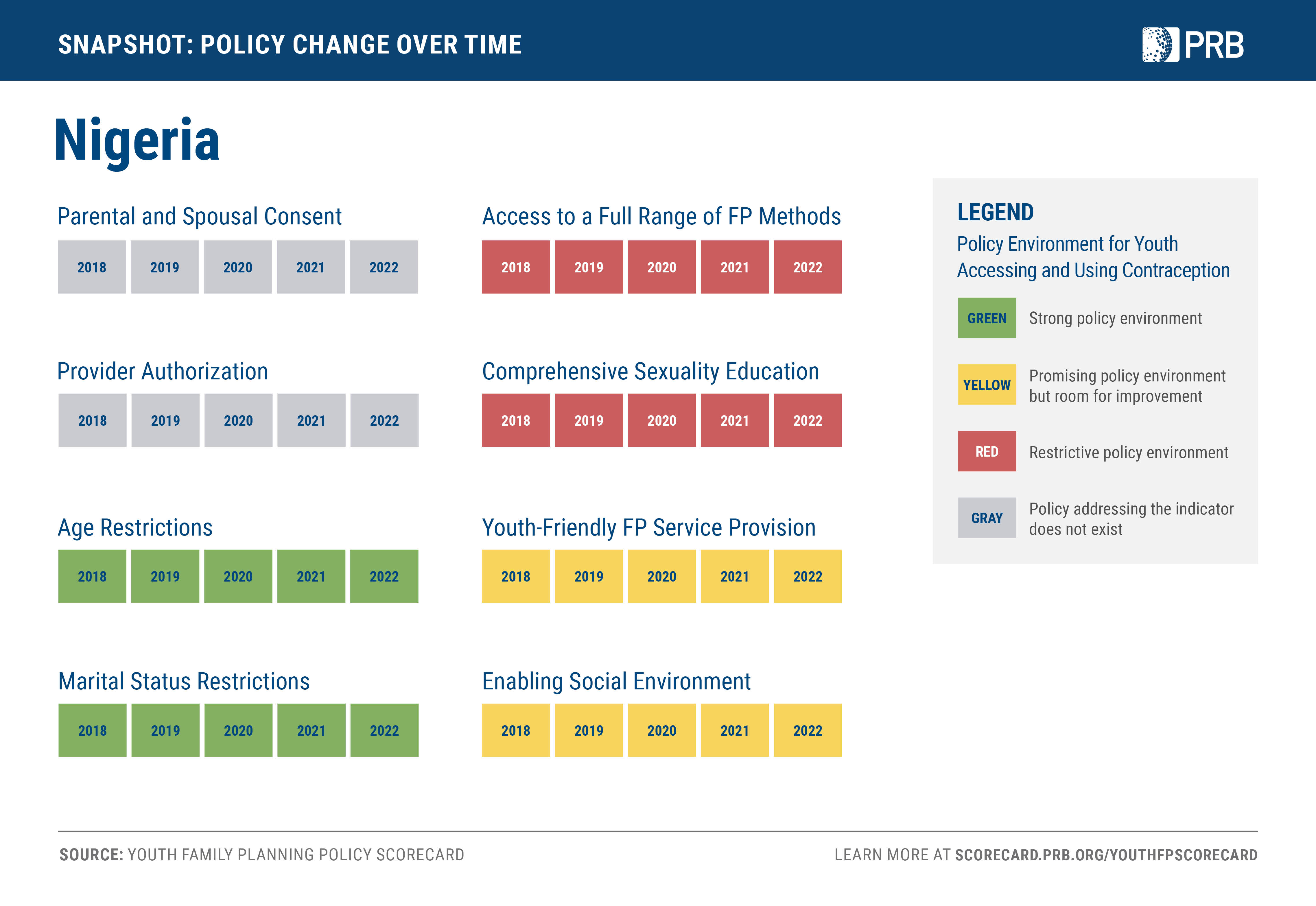{kind=link}
{kind=link}
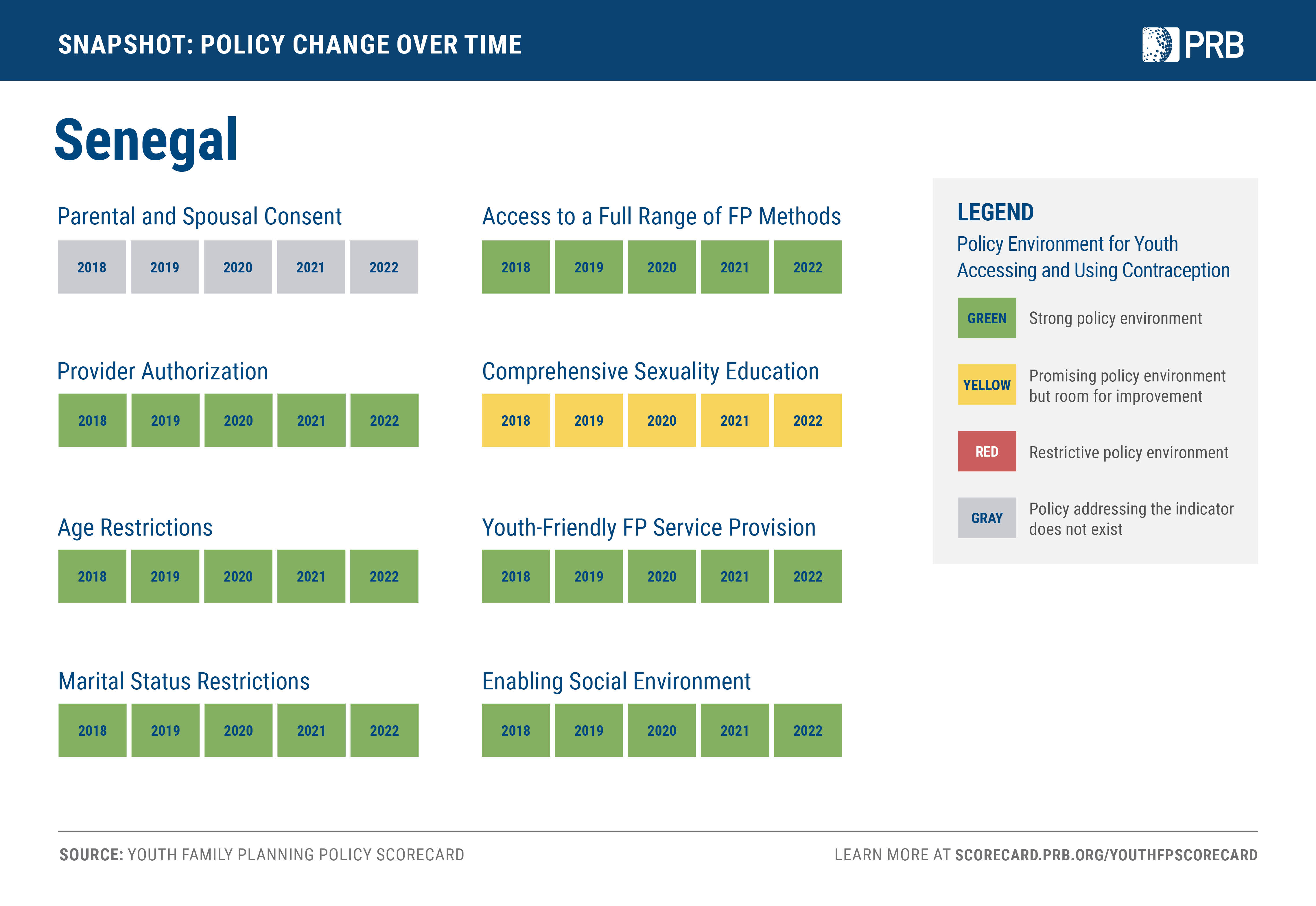{kind=link}
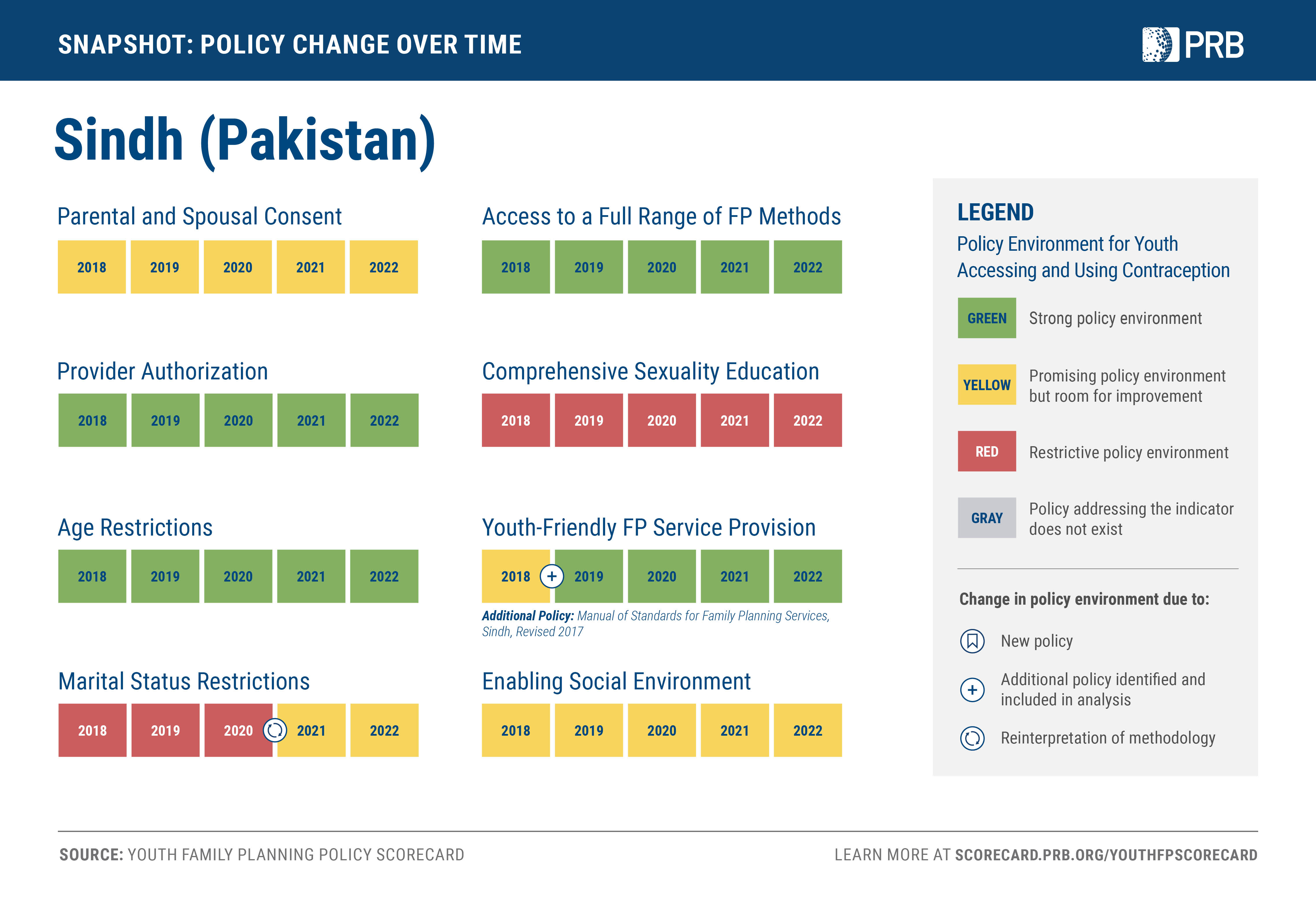{kind=link}
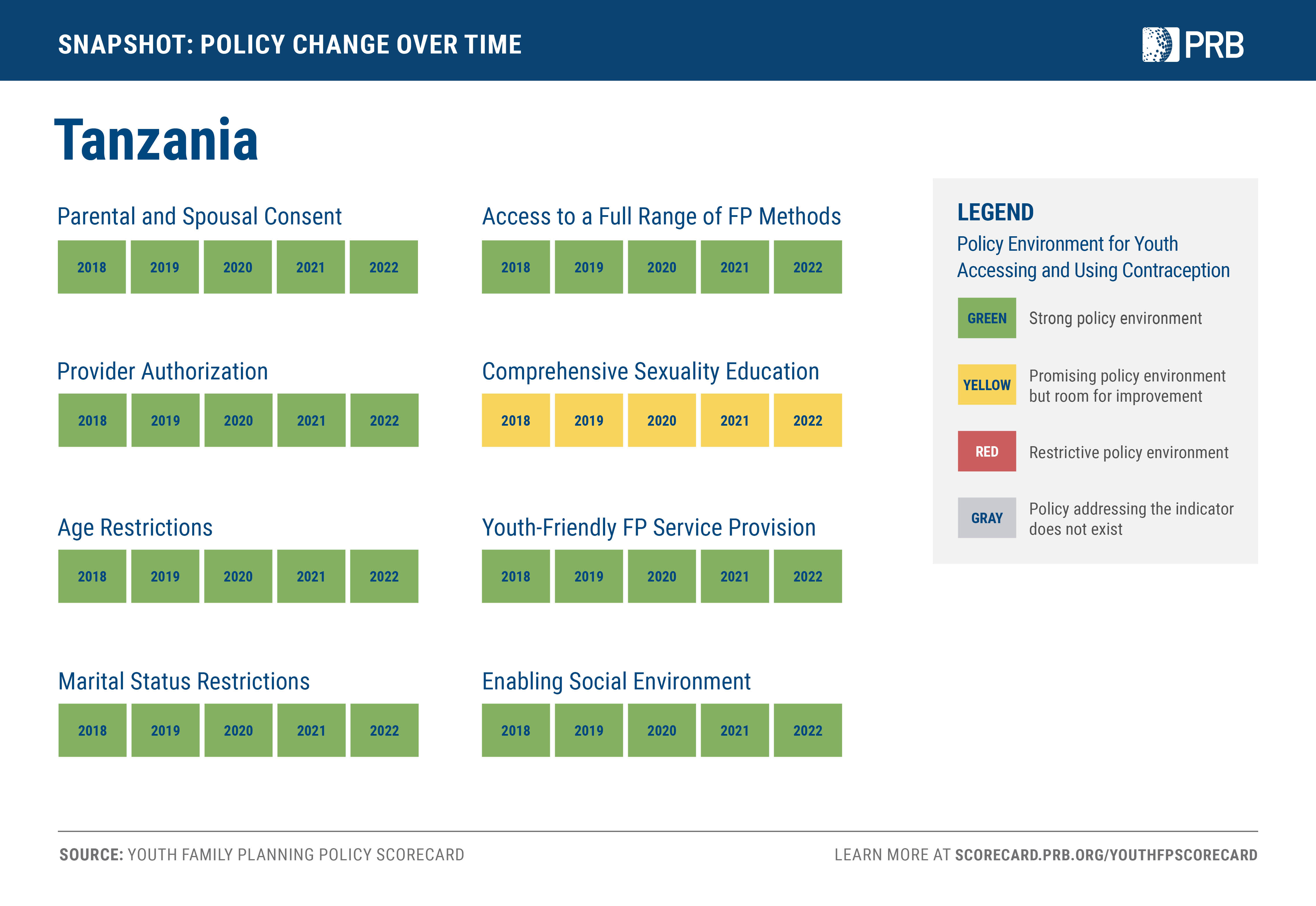{kind=link}
{kind=link}
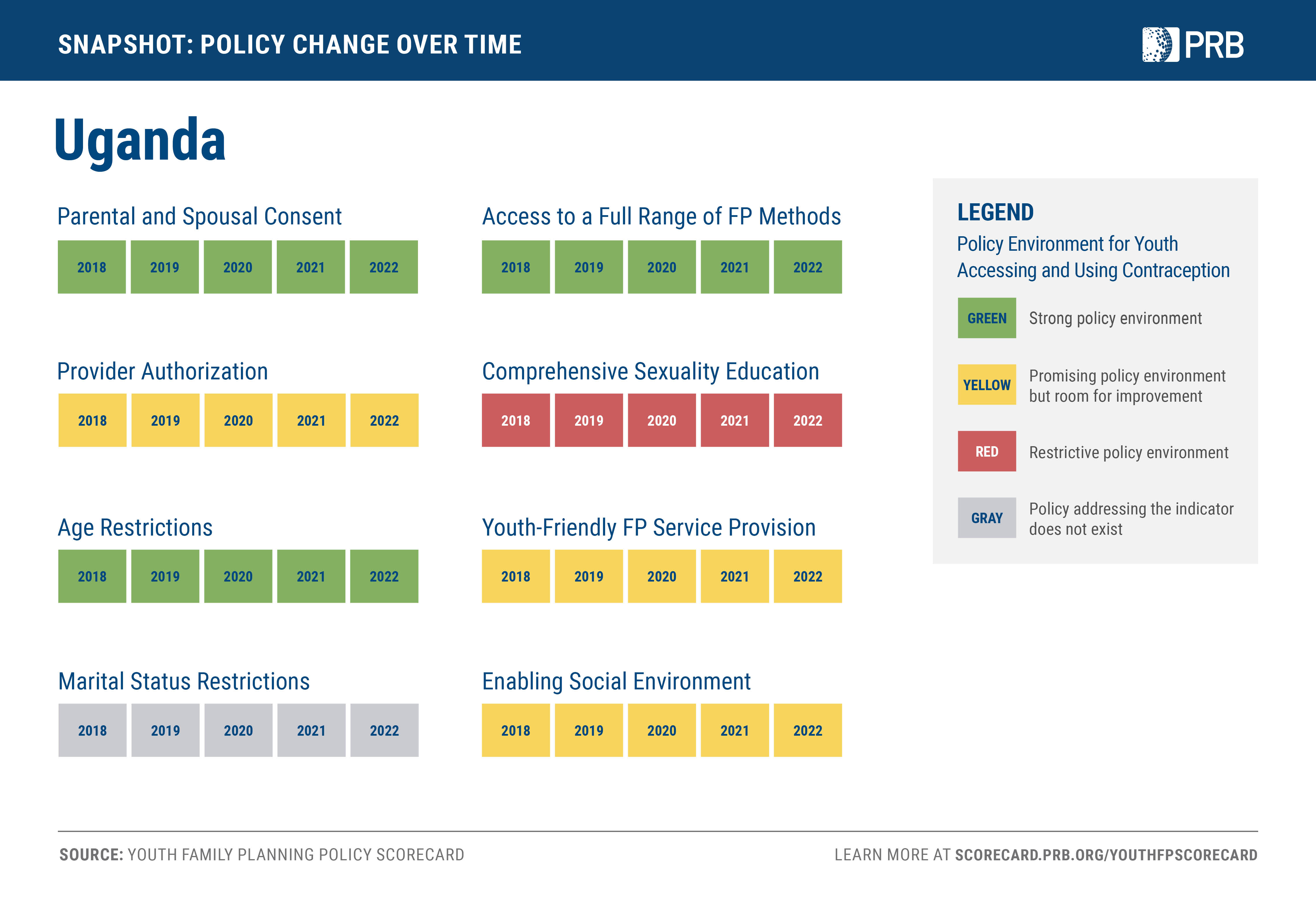{kind=link}
{kind=link}